

Byline: Eleanor Markham
The most important public health policy lesson of the past generation is also the least comfortable for governments to accept. Health systems don't secure population health by treating illness efficiently after it appears. They do so by preventing exposure to risk in the first place. In the UK, deaths from acute myocardial infarction and stroke fell by 40% over a 30-year period, and 58% of that decline was attributed directly to changes in risk factors, primarily reduced smoking prevalence, not only to medical treatment improvements, according to analysis published in the BMJ archive.
For G7 and G20 leaders, that finding should alter the policy frame. Resilient systems aren't defined only by hospital capacity, emergency stockpiles, or new technologies. They're defined by whether governments can align law, finance, data, regulation, and political accountability around prevention. That means confronting the structural and commercial drivers of ill health, not just expanding service delivery once damage has already been done.
Table of Contents
- Defining the Mandate for Public Health Policy in 2026
- The Modern Framework for Effective Health Policy
- Five Key Levers for Policy Action
- Navigating Health Governance from National to Global Arenas
- Lessons from Landmark Public Health Interventions
- The Unseen Driver Commercial Determinants of Health
- A 2026 Roadmap for Resilient and Equitable Health Systems
Defining the Mandate for Public Health Policy in 2026
Public health policy in 2026 isn't a niche administrative function. It's a core instrument of state capacity. Governments that still treat prevention as discretionary spending are effectively choosing higher downstream costs, weaker labour force participation, and more fragile social cohesion.
The clearest warning sign is legal, not clinical. The Faculty of Public Health's 2024 vision calls for a £1 billion real-term restoration of the Public Health Grant and argues that without statutory enforcement to make prevention a core NHS duty, the system can't reverse the growing 10-year diagnosis gap between the most and least deprived communities, as set out in its vision for the public's health. That diagnosis gap should matter far beyond the UK. It shows what happens when prevention is rhetorically praised but institutionally optional.
Public health policy fails when prevention depends on goodwill rather than law.
For G7 and G20 governments, the mandate is broader than domestic service reform. Pandemic preparedness, climate-linked health risks, antimicrobial resistance, demographic ageing, food systems, migration, urban resilience, and data governance all converge in the same policy arena. Ministries still tend to divide these questions into separate silos. Populations don't experience them that way.
A durable mandate rests on three propositions:
- Prevention is strategic infrastructure: It reduces pressure on hospitals, labour markets, and public finances before crises mature.
- Inequality is a governance issue: Health gaps reflect legal design, commercial incentives, and institutional priorities, not only individual behaviour.
- Multilateral credibility begins at home: Countries can't lead globally if national systems still reward treatment while underfunding prevention.
That last point is often missed in summit diplomacy. Leaders speak comfortably about resilience. Fewer are willing to redesign statutory duties, budget rules, and regulatory frameworks so that resilience becomes operational. That's where public health policy moves from aspiration to statecraft.
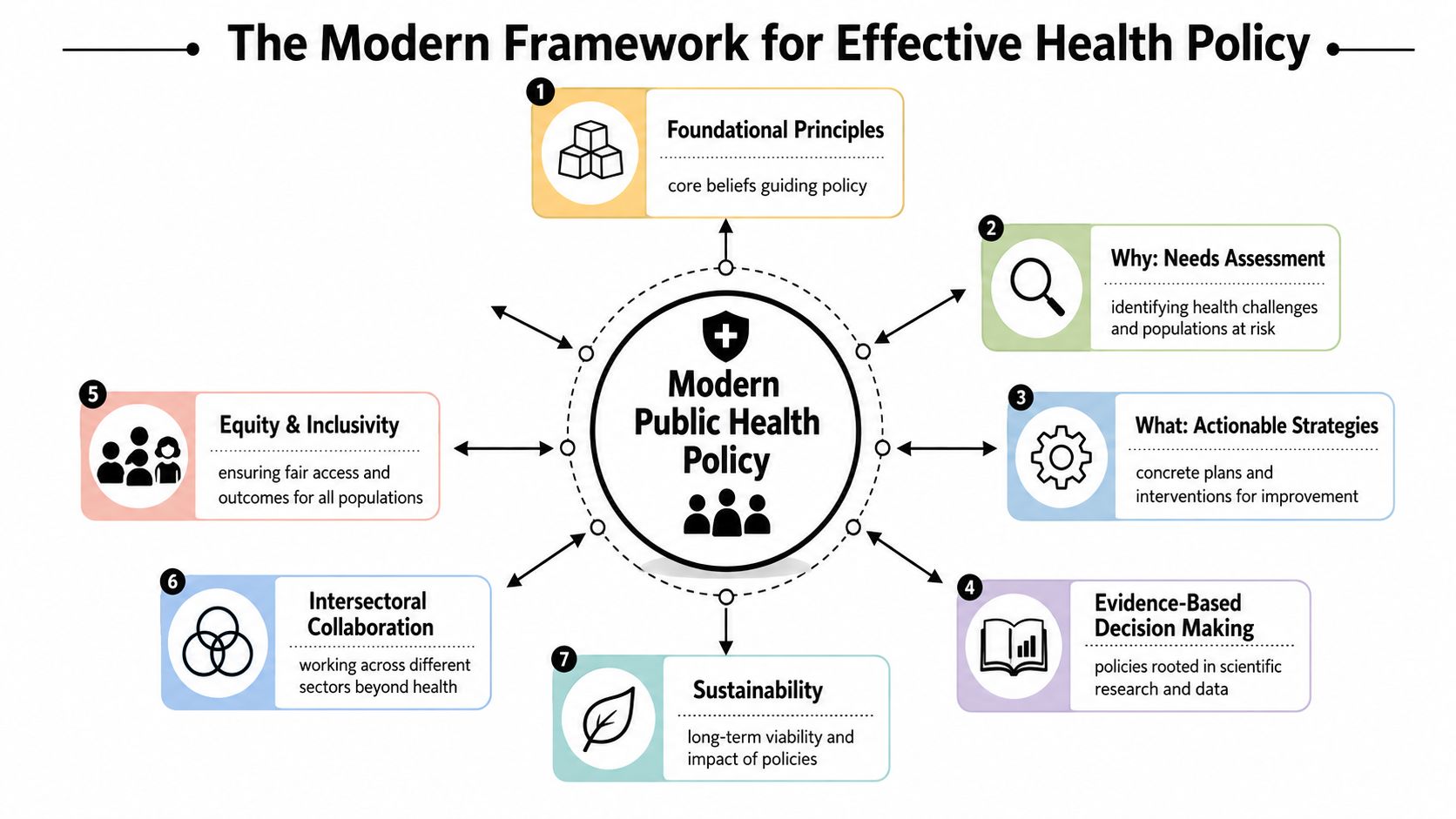
The Modern Framework for Effective Health Policy
Modern public health policy should be judged less by intent than by method. Good intentions are abundant in health policy. Credible design is rarer.
Evidence before assertion
In England, public health policy development must follow a formal evidence-based framework. That framework requires policymakers to prove both the existence of a health problem and the likely positive outcome of an intervention using the “best available evidence”, defined as credible, reliable, accurate, and authoritative, before a policy can be asserted, as described in this analysis of evidence use in English public health policymaking.
That standard matters because health policy often drifts into one of two errors. The first is symbolic action, where governments announce a measure because it signals concern. The second is technocratic overconfidence, where officials assume that more data automatically means better policy. Neither is enough. Evidence has to be directly related to the claim at hand, and it has to support a plausible route from intervention to outcome.
A practical framework for ministers and senior officials includes the following tests:
| Test | Question for decision-makers |
|---|---|
| Problem test | Is the health problem clearly established with credible evidence? |
| Intervention test | Is there a reasoned basis to expect the policy to improve outcomes? |
| Distribution test | Who benefits first, and who may still be left behind? |
| Delivery test | Which institution is accountable for implementation and monitoring? |
| Legitimacy test | Does the policy align with existing legal duties and public expectations? |
Law and legitimacy
Evidence alone doesn't create durable policy. Legal architecture does. Public health policy gains traction when it's anchored in formal duties, enforceable powers, and institutional accountability. It weakens when prevention is treated as an advisory preference.
The legal dimension also has an international edge. National policy has to align with domestic health law and wider obligations that shape how states justify intervention, coordinate surveillance, and manage cross-border risks. For G7 and G20 leaders, that means a strong framework must combine four elements:
- Credible evidence: not anecdote, not trend-chasing
- Equity by design: not as an annex, but as a criterion in policy selection
- Cross-sector reach: because food, transport, housing, trade, and education shape health outcomes
- Institutional durability: so prevention survives electoral turnover and fiscal tightening
Operational principle: If a policy can't explain its evidence base, legal basis, and equity impact, it isn't ready for scale.
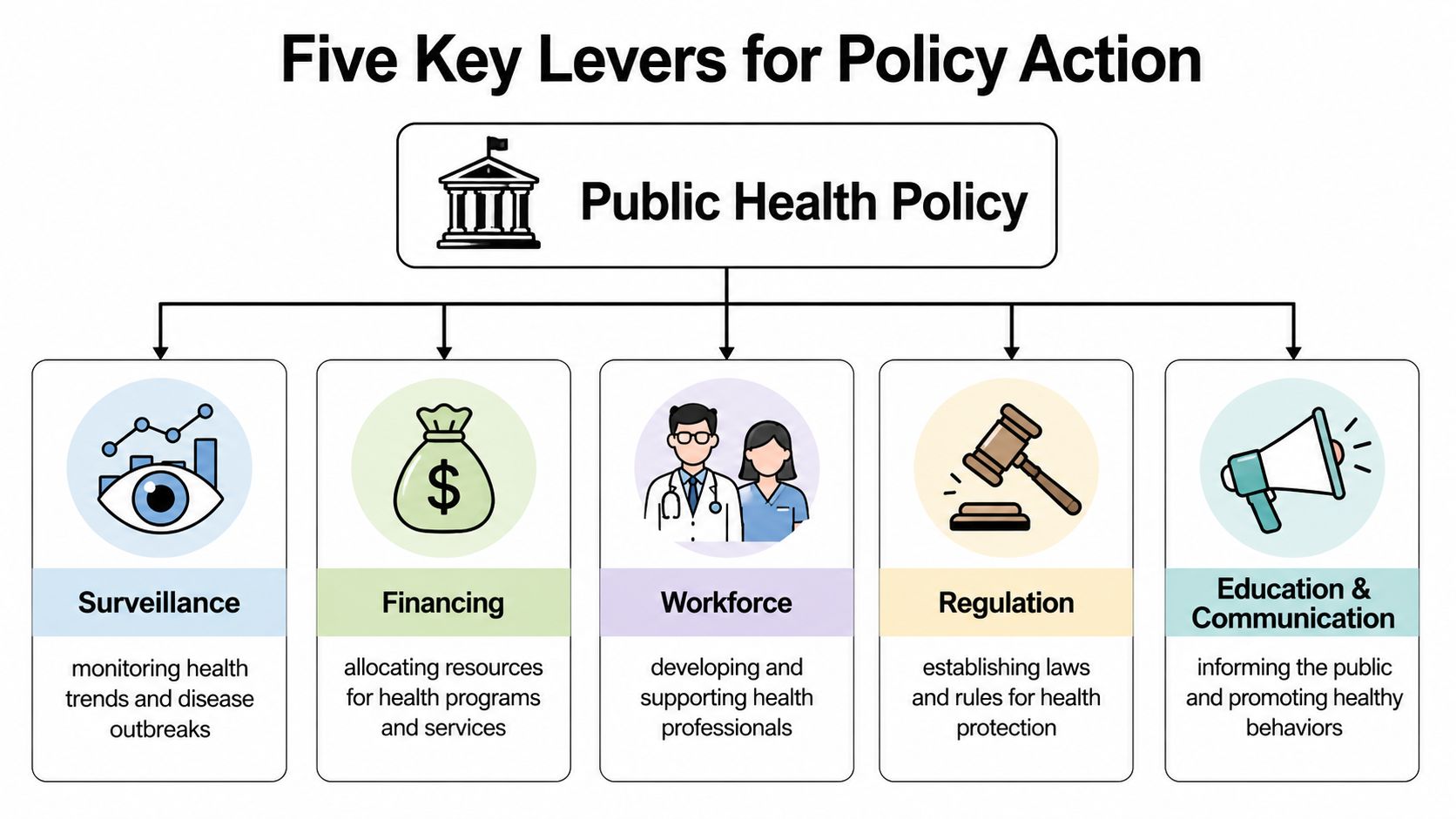
Five Key Levers for Policy Action
Public health policy becomes actionable when leaders stop treating it as a single sector and start managing it as a toolkit. In practice, five levers matter most: surveillance, financing, workforce, regulation, and equity-oriented design.
How the levers work in practice
Surveillance is more than outbreak monitoring. It's the state's capacity to detect, interpret, and act on population-level signals. The UK has committed up to £200 million to NHS data infrastructure, with secure data environments established as the default route for research access, and all data sharing arrangements required to have an explicit aim to improve patient health or NHS operations, according to this summary of the UK's national strategy for health data. That is the right direction. Surveillance becomes politically legitimate when data access is linked clearly to public value and governed securely.
Financing determines whether prevention survives beyond press conferences. Many countries still fund public health in a residual way, boosting budgets during emergencies and retrenching afterwards. That model guarantees volatility. More durable approaches ringfence core capability, tie budget decisions to long-term risk reduction, and connect public health spending to wider fiscal strategy. The debate on financing universal health coverage is relevant here because service coverage without preventive capacity isn't financially stable.
Workforce is often discussed as a staffing issue. It's a capability issue. Public health systems need epidemiologists, behavioural scientists, inspectors, data specialists, local delivery teams, and policy professionals who can negotiate across ministries. A workforce plan that focuses only on clinical roles will leave major preventive functions underpowered.
A ministerial test for readiness
Regulation and equity require different instincts from the first three levers. They're about choices governments make in the face of competing interests.
- Regulation shapes markets: Tobacco control, alcohol pricing, food standards, advertising rules, and smoke-free laws don't merely inform behaviour. They alter the environment in which behaviour occurs.
- Equity changes targeting: It asks whether an intervention reaches populations facing the earliest and heaviest burden of illness.
- Implementation matters more than announcement: A regulation without enforcement is a signalling device, not a policy instrument.
A simple readiness screen can help cabinets assess whether a proposed measure is serious enough to proceed:
- Can the state observe the problem? If not, strengthen surveillance first.
- Can the measure be funded over multiple budget cycles? If not, it isn't system reform.
- Does the workforce exist to execute it locally? If not, national ambition will stall.
- Can regulation change incentives upstream? If not, the policy may only manage symptoms.
- Will the design narrow disparities, or improve averages? If leaders can't answer this, they're governing blind.
The value of this five-lever model is strategic. It prevents governments from overinvesting in one instrument, usually healthcare delivery, while neglecting the others that determine whether population health improves at scale.
Navigating Health Governance from National to Global Arenas
Health governance is often described as if it were a ladder. Local, national, regional, global. In reality, it behaves more like a loop. Local implementation exposes problems, national systems codify solutions, regional networks spread practice, and global institutions set norms that flow back into domestic reform.

National architecture matters
The legal structure of national systems determines whether health governance is coherent or fragmented. In the UK, the Health and Care Act 2022 placed Integrated Care Systems on a statutory footing, enabled NHS England to define mandatory data specifications, criminalised inappropriate data sharing, and explicitly permitted NHS Digital to share information for healthcare, social care, and research purposes, as examined in BMJ Open's review of the changing legal environment for health data governance. That matters because governance failures usually arise from ambiguity. Who holds the data. Who may use it. Who is accountable for outcomes. Who can coordinate across organisational boundaries.
Integrated structures won't solve every problem. But they create a decision space where prevention, care delivery, social care, and population-level planning can be aligned rather than negotiated ad hoc.
The quality of health governance depends less on organisational charts than on whether duties, permissions, and accountability lines are clear enough to support action.
What multilateral forums should actually do
Global forums shouldn't attempt to run national health systems. Their role is different. They should set common priorities, reduce coordination costs, and create political pressure for implementation. That's where the G7 and G20 can add value, especially when translating broad health commitments into interoperable standards on data, preparedness, regulation, financing, and accountability.
A useful reference point is the wider conversation on global health initiatives. The challenge for summit diplomacy isn't producing another declaration. It's building mechanisms that help national ministries convert commitments into routine administrative practice.
For decision-makers, the governance hierarchy is best understood as a division of labour:
| Level | Primary function |
|---|---|
| Local | Deliver programmes, monitor community effects, adapt implementation |
| National | Legislate, finance, regulate, and integrate systems |
| Regional | Coordinate shared risks and policy learning |
| Global | Set norms, broker cooperation, and sustain political momentum |
Where this breaks down, prevention usually suffers first. Treatment has visible constituencies and immediate pressures. Prevention needs institutions that can hold a line over time.
Lessons from Landmark Public Health Interventions
Public health succeeds when governments reshape the conditions that produce risk, not only when health services treat its consequences. The historical record shows that the largest gains have come from interventions that changed markets, environments, and everyday behaviour at population scale.
A useful case is tobacco control. The WHO Framework Convention on Tobacco Control established a policy package that combined taxation, advertising restrictions, smoke-free rules, health warnings, and measures against industry interference. WHO's summary of the treaty's impact shows how countries used these tools to reduce tobacco use and shift social norms over time, rather than relying on one-off campaigns or clinical advice alone in its Framework Convention on Tobacco Control overview. The lesson for G7 and G20 leaders is operational. Durable health gains usually follow policy layering across fiscal, regulatory, and communications systems.
Immunisation offers a second lesson. Smallpox eradication was not a triumph of vaccine availability by itself. It depended on surveillance, targeted containment, field operations, and international coordination under a common strategy, as documented in the WHO account of the history of smallpox eradication. Food safety reform follows the same logic. Outcomes improve when inspection, reporting, product standards, and enforcement work together, not when governments issue advice without changing the incentives and obligations facing producers.
These cases point to a pattern that current policy debates often miss. The most effective interventions addressed structural drivers upstream. They altered what firms could sell, how products were marketed, which risks were tolerated in public spaces, and how quickly authorities could detect and contain harm. That is why public health history matters for present-day strategy. It shows that prevention is strongest when policy reaches beyond the clinic and into the commercial and regulatory systems that shape exposure in the first place.
Three lessons stand out for decision-makers:
- Long time horizons are a policy asset: Major reductions in risk usually come from sustained implementation, not short funding cycles or ministerial relaunches.
- State capacity matters as much as policy design: Surveillance, inspection, procurement, and enforcement determine whether formal commitments change real-world exposure.
- Commercial incentives must be part of the intervention model: Where profits depend on harmful consumption or weak safety standards, voluntary action rarely produces population-level protection.
Current leaders should read these lessons against the shock delivered by the effects of Covid on the medical field. The pandemic exposed what happens when countries underinvest in prevention infrastructure and allow supply resilience, workforce stability, and public communication capacity to erode. The practical conclusion is straightforward. Health systems become more resilient when governments treat prevention as an economic governance function, not a peripheral social programme.
The Unseen Driver Commercial Determinants of Health
Many health debates still revolve around a false binary. Either poor outcomes are driven by poverty, or they're driven by weaknesses in healthcare access. Both matter. But that frame misses a third force that policymakers can act on more directly: the commercial determinants of health.
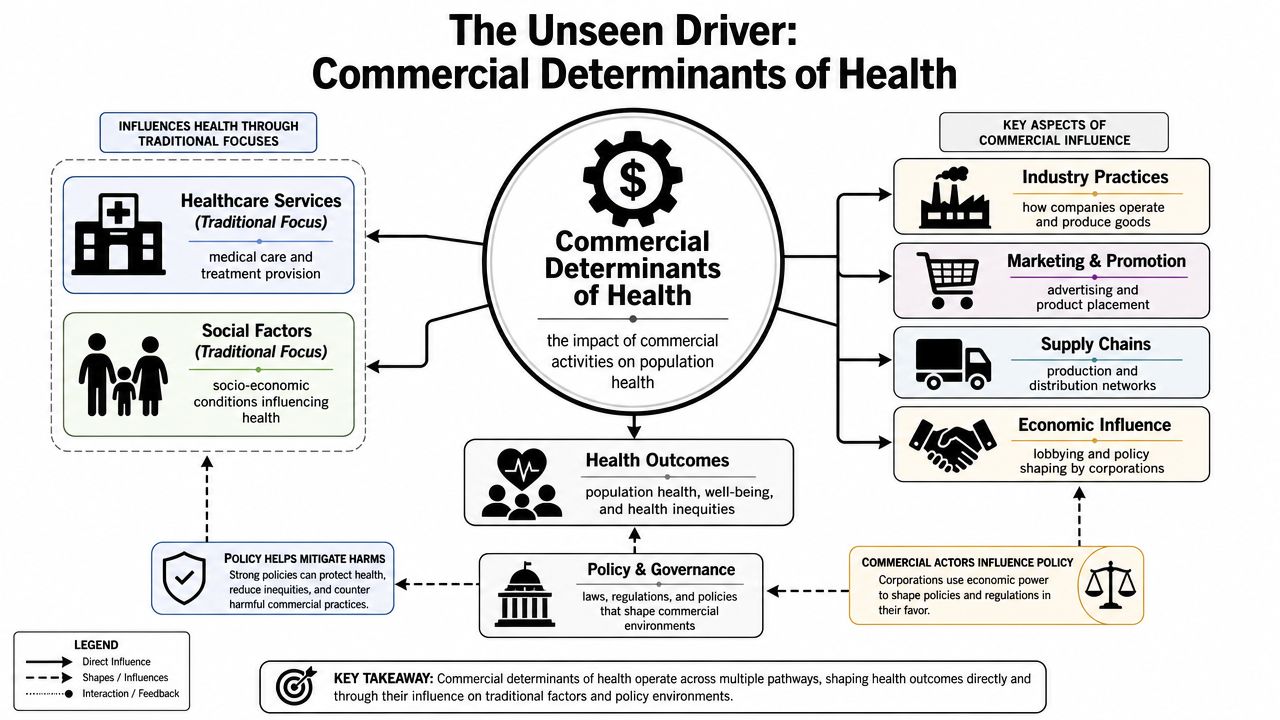
Why the standard debate is too narrow
The Association of Directors of Public Health argues that governments must implement policies against commercial determinants linked to smoking, alcohol, and unhealthy food, and notes that people in the most deprived parts of England are diagnosed with major illness 10 years earlier than people in the least deprived areas, as stated in its 2023 health inequalities policy position statement. That's the policy hinge. If harmful consumption patterns are shaped in part by marketing, pricing, availability, product formulation, and lobbying, then public health policy that ignores these drivers will remain incomplete.
This changes how leaders should interpret inequality. Deprivation doesn't just create vulnerability. It also creates markets. Industries selling harmful products often concentrate exposure where regulation is weaker, purchasing power is constrained, and stress is already high. A health system can treat the consequences, but it can't regulate away upstream harm from inside the clinic.
A prevention strategy that doesn't confront commercial incentives will improve services while leaving the production of ill health largely intact.
What a commercial determinants approach changes
A commercial determinants lens leads to a different policy repertoire.
- Advertising and promotion rules become health tools, not only consumer protection measures.
- Pricing policy becomes preventive architecture, particularly for tobacco and alcohol.
- Procurement and food standards become part of chronic disease strategy.
- Cross-government oversight becomes essential because trade, treasury, education, and business policy all shape exposure.
Many governments still underperform by supporting equity rhetorically while tolerating market conditions that intensify inequality materially. For G7 and G20 leaders, that's a strategic blind spot. If summit commitments focus only on hospitals, insurance, and innovation, they'll miss one of the most actionable drivers of poor health outcomes.
A 2026 Roadmap for Resilient and Equitable Health Systems
The next phase of public health policy needs fewer declarations and more hard wiring. G7 and G20 leaders should focus on a compact set of decisions that change institutional behaviour.
Six decisions for G7 and G20 leaders
First, make prevention a statutory duty inside health systems. Where prevention is optional, treatment will dominate because it is immediate, visible, and politically harder to defer.
Second, restore and protect long-term public health financing. Short budget cycles are poorly matched to long-horizon gains. Prevention requires stable institutional memory, not intermittent rescue packages.
Third, create cross-government mechanisms to address commercial determinants of health. A ministerial committee with authority across health, treasury, education, food, and trade is more useful than another standalone strategy document.
Fourth, invest in trusted, privacy-protective data systems that support both preparedness and public legitimacy. Data access should be fast enough for policy use and governed tightly enough to retain consent and confidence.
Fifth, treat equity as a design rule. That means targeting earlier diagnosis, earlier intervention, and easier access in places where illness arrives sooner and compounds faster. Practical debates on maternal and community-based care also belong here. For example, the evolving map of states covering doula services 2026 is useful because it shows how policy design can widen or narrow access depending on reimbursement and implementation choices.
Sixth, use multilateral forums to lock in interoperability rather than rhetoric. Leaders should align around practical standards for surveillance, workforce cooperation, emergency coordination, and prevention-focused financing. The broader strategic case for this is clear in discussions of the G20's role in ensuring global health security.
From summit language to delivery systems
A resilient health system isn't one that merely recovers from shocks. It's one that reduces the frequency, intensity, and inequality of those shocks before they reach crisis point.
That requires a political shift. Leaders need to stop asking whether they can afford prevention and start asking whether their current model can survive without it. On the available evidence, it can't. The countries that perform best over the next decade won't be those with the most impressive emergency response language. They'll be the ones that legislate prevention, regulate commercial harm, finance public health consistently, and connect national delivery to global cooperation.
Global Governance Media helps decision-makers turn that agenda into action with analysis grounded in multilateral realities, summit priorities, and practical policy choices. Explore Global Governance Media for informed coverage of G7 and G20 health governance, resilience, and prevention-led reform.