

By Daniel Mercer
The most revealing fact about funding for NIH isn't only its size. It's where that money goes, how it moves, and what happens internationally when that movement slows. In FY 2025, the NIH received $48.5 billion in appropriations and awarded $35.3 billion in competing and noncompeting grants, according to the University of Pennsylvania LDI summary of NIH funding trends. For any government, university, hospital network, or multilateral health actor working across borders, that scale makes NIH funding part of the operating environment, not just a US domestic budget line.
That matters because NIH decisions shape the tempo of vaccine research, clinical trials, lab partnerships, shared datasets, and scientific careers well beyond the United States. UK universities, NHS-linked research centres, European consortia, and global health institutions often collaborate with NIH-funded teams or compete within a wider research market influenced by NIH priorities. When the NIH expands, contracts, or reallocates, those effects ripple through transatlantic science.
Most commentary on funding for NIH still treats the subject as an application guide. That misses the more strategic question. NIH funding is also a map of state capacity, political priorities, and institutional concentration. It tells policymakers where biomedical power sits, which missions Washington protects, and where access gaps persist despite the rhetoric of open competition.
This article takes that broader view. It looks at the politics behind appropriations, the internal machinery that turns Congressional funding into grants, the pressures now visible in award data, and the geography of US biomedical investment. The last of these deserves far more attention in UK and international policy debates than it currently receives.
For readers following global health initiatives and cross-border policy coordination, the central point is simple. NIH funding isn't just a line in the US federal budget. It's infrastructure for the wider global research system.
Table of Contents
- Introduction: Why NIH Funding Matters on the Global Stage
- The Engine Room: Federal Appropriations and Political Drivers
- Anatomy of a Budget: NIH Structure and Institute Allocations
- From Policy to Practice: Grant Mechanisms and Key Programmes
- Currents and Headwinds: Recent NIH Funding Trends and Data
- The Geography of Innovation: Funding Disparities and Global Lessons
- Conclusion: Policy Pathways for a Resilient Global R&D Ecosystem
Introduction: Why NIH Funding Matters on the Global Stage
Funding for NIH has become shorthand for a larger question. Who sets the pace of biomedical research in an era when health security, industrial policy, and strategic competition are increasingly fused together?
The NIH sits at the centre of that question because of its role as a public financer of basic, translational, and clinical research. Its influence isn't limited to the grants it signs directly. It also shapes norms around peer review, signals which disease areas gain prestige, and affects how universities structure laboratories, recruit staff, and build long-term collaborations. For international partners, NIH funding often functions like an anchor institution in the global science economy.
Why scale changes the policy meaning
A budget on this scale does more than support individual projects. It creates a market for talent, equipment, data infrastructure, and trial networks. That's why shifts in funding for NIH can alter incentives even for institutions that never apply directly. When US biomedical funding expands, researchers elsewhere often benefit through partnerships and shared platforms. When it tightens, those same institutions face delays, narrower consortium options, and greater uncertainty.
Policy insight: International actors should treat NIH appropriations as an external determinant of their own research resilience, not as a distant American issue.
The global relevance is strongest in fields where scientific cooperation depends on expensive infrastructure and sustained data sharing. Infectious disease surveillance, oncology, genomics, and rare disease research all rely on institutional continuity. In those areas, predictable NIH support helps stabilise cross-border collaboration.
Why policymakers should care about the mechanics
A second reason NIH funding matters globally is that it reveals how a major democracy translates political choice into research capacity. That process is messy by design. Appropriations are negotiated, institutional missions compete, and targeted programmes carve out space for specific priorities. But those details matter. They show whether a research system rewards long-range planning or forces institutions into short budgeting cycles.
For UK and European policymakers, the lesson isn't to copy the NIH model wholesale. It's to read it carefully. The structure of funding shapes scientific geography, career incentives, and international bargaining power. Those are strategic issues, not administrative ones.
The Engine Room: Federal Appropriations and Political Drivers

A single annual appropriations decision in Washington helps determine whether biomedical capacity concentrates further in Boston, San Diego, and the Bay Area, or whether more of the United States develops the laboratory base needed to contribute to national and international research networks. That is the larger significance of funding for NIH. The budget is not only a science figure. It is a territorial policy signal.
How the budget becomes real money
NIH spending begins with the president's budget request, but Congress determines the final appropriation through committee markups, negotiations across both chambers, and wider bargaining over federal spending caps. Universities, teaching hospitals, patient groups, medical charities, and industry associations all try to shape that outcome. The final number reflects political compromise rather than a neutral assessment of scientific opportunity.
The broad trend is familiar even without revisiting the data cited earlier in this article. NIH purchasing power has not risen in a straight line, and periods of apparent growth in nominal dollars have often masked pressure in real terms. For laboratories, that distinction is practical. Staff costs rise, equipment ages, compliance requirements expand, and advanced computing infrastructure absorbs a larger share of fixed budgets.
The distributional effect inside the United States receives less attention than the topline figure. Large, research-intensive states are better positioned to absorb uncertainty because they already have grant offices, experienced principal investigators, and hospital systems that can bridge temporary funding gaps. Smaller or historically underfunded states have less room to do that. Annual appropriations therefore shape not only how much science the US can support, but where that science can plausibly happen.
That point has wider relevance.
Political incentives shape scientific geography
Appropriators respond to several overlapping pressures, and each has implications for regional concentration.
- Crisis visibility: Epidemics and other public health shocks can produce short bursts of political support, often directed toward immediately legible threats rather than slower capacity building.
- Advocacy density: Elite universities, major academic medical centres, and well-organised disease groups can press their case more consistently than regions with thinner institutional representation.
- Fiscal constraint: NIH may retain bipartisan goodwill, but goodwill does not remove competition with defence, entitlement spending, or deficit politics.
These drivers matter internationally because they influence whether the US research system broadens participation or reinforces existing clusters. A funding system that repeatedly rewards places with established scale can produce scientific excellence, but it can also narrow the domestic map of expertise. That has consequences for resilience. If advanced capacity is concentrated in a limited number of metropolitan hubs, the system becomes more exposed to local labour shortages, infrastructure bottlenecks, and political backlash from regions that feel excluded from national innovation gains.
For analysts examining the political incentives behind public spending choices, NIH appropriations offer a useful case. Budget design, coalition strength, and committee politics affect which institutions can plan for ten years and which must budget year to year.
Why this matters beyond the United States
For foreign ministries, UK research funders, and multilateral health institutions, the appropriations cycle is not a distant domestic ritual. It shapes which US partners can sustain trial sites, host shared data platforms, or enter long-horizon collaborations on credible terms. It also indicates whether the American system is reproducing a narrow set of research regions or building a broader national base that can support more diversified international partnerships.
That second question should matter in Britain and Europe. Debates over place-based R&D funding often focus on national productivity, regional inequality, or university finance. NIH shows that the same debate is also about international capacity. Countries that concentrate public research money in a few superstar regions may gain efficiency at the frontier, yet they also limit the number of places able to plug into global consortia, absorb external shocks, and contribute to distributed preparedness.
Stable health research partnerships depend on stable appropriations, but they also depend on a wider domestic spread of research capacity.
The policy lesson is sharper than a standard NIH explainer usually allows. The key issue is not only whether Congress funds biomedical science generously. It is whether federal appropriations, taken together with political incentives, widen or narrow the geography of American research. For allies designing their own biomedical strategies, that is the more transferable lesson.
Anatomy of a Budget: NIH Structure and Institute Allocations
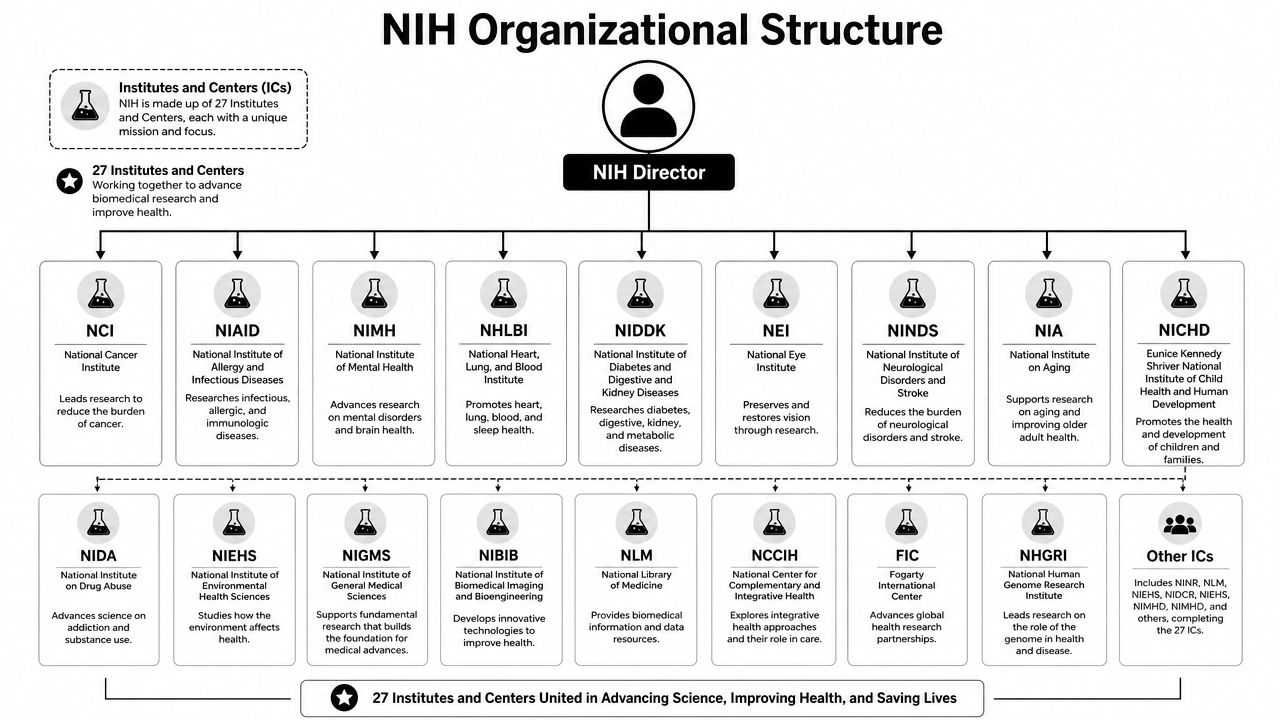
The NIH doesn't operate as a single monolithic agency in practice. It functions more like a federation of mission-based entities housed under one umbrella. That distinction matters because funding for NIH is allocated through a structure that channels resources into distinct scientific domains, each with its own priorities, review culture, and portfolio logic.
A federation rather than a single pot
A useful analogy is a large corporation with multiple specialised divisions. The NIH Director sits at the top, but the actual distribution of research money depends heavily on the Institutes and Centres. Each one focuses on a defined mission area, and applicants usually engage with those mission boundaries rather than with “NIH” in the abstract.
For policymakers outside the United States, this internal architecture is often the missing piece. Collaboration opportunities, review expectations, and programme fit vary across the NIH structure. A university or research ministry looking at funding for NIH as one large pool will misunderstand how decisions get made. The practical unit of analysis is usually the relevant Institute or Centre.
Why RePORT matters for policy analysis
The best way to understand that structure is through the NIH's own public data systems. The NIH RePORT and RePORTER databases provide granular public access to historical spending categories, success rates, and grant awards, making them valuable tools for analysing allocation patterns across Institutes and Centres with precision, as described on the NIH RePORT funding portal.
That matters for more than transparency. It allows analysts to move beyond headline spending and ask harder questions:
- Which mechanisms dominate? A portfolio can look broad while becoming concentrated in a narrow set of award types.
- Where is volatility highest? Some parts of NIH may experience sharper year-on-year instability than others.
- How much money follows mission-led priorities? Funding concentration can signal changing strategic priorities even without a dramatic top-line shift.
A UK research office or health department can use these data to benchmark US priorities against its own choices. That's especially useful when judging whether collaboration should be built around infectious disease, cancer, minority health, or platform technologies.
Practical rule: Don't analyse NIH from the top line alone. The strategic signal sits lower down, inside the Institutes, award mechanisms, and mission-specific allocations.
The structure also explains why NIH can appear simultaneously centralised and fragmented. Central political oversight exists, but operational power is distributed. That gives the system flexibility. It can also make it harder for external partners to predict how broad federal priorities will translate into institute-level funding opportunities.
From Policy to Practice: Grant Mechanisms and Key Programmes
Funding for NIH only becomes meaningful when it reaches research teams. That happens through grant mechanisms that embody different policy goals. Some reward established lines of inquiry. Others create room for riskier ideas, infrastructure building, or targeted mission delivery. The grant architecture matters because it decides not just who gets funded, but what type of science becomes institutionally possible.
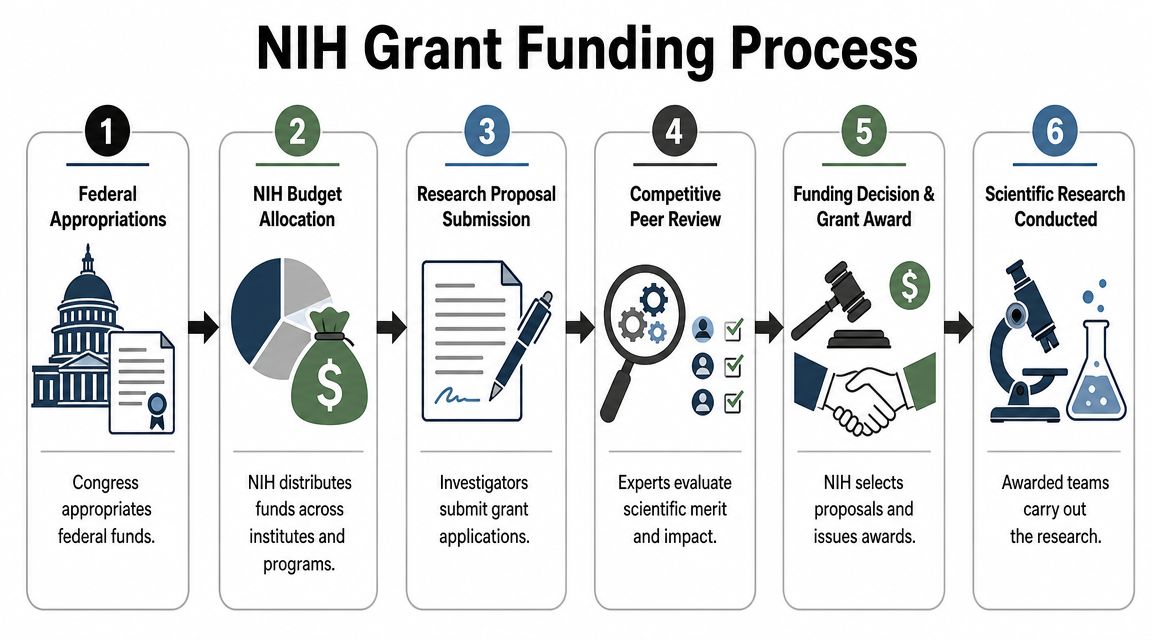
How NIH money reaches researchers
The standard pathway is competitive and peer reviewed. Funds move from federal appropriations to institute budgets, then into specific opportunities and investigator-led applications. Peer review remains a core part of the system because it gives technical experts a formal role in sorting proposals by scientific merit and feasibility.
A simple visual summary helps.
The best-known mechanism is the R01, often treated as the benchmark investigator-initiated research award. The R21 serves a different function, backing exploratory or developmental work where the case for innovation may be stronger than the case for certainty. That distinction matters for applicants, but it also matters for policymakers. Mechanism mix shapes whether a system favours cumulative science, high-risk experimentation, or narrowly targeted delivery.
For international institutions, one practical implication stands out. If a government wants its universities to partner effectively with US counterparts, it needs administrative literacy about NIH mechanisms, programme fit, and timing. Institutions that lack that literacy may have excellent science and still struggle to position themselves.
That's one reason debates about public-health R&D advocacy and strategic positioning shouldn't stop at top-line budget support. They also need to address how applicants interact with the machinery beneath the budget.
Targeted missions and equity funding
The NIH funds broad science, but it also uses targeted appropriations to protect specific missions. One clear example is the National Institute on Minority Health and Health Disparities, which had an FY2025 appropriation of $535.14 million, according to the NIH grants and funding information page. That figure matters because it shows how part of the NIH budget is reserved for a defined equity-oriented mission rather than being absorbed into general competition.
For UK and international readers, this raises a sharper policy question than most NIH explainers ask. How much of a biomedical funding system is open-ended, and how much is carved out to address recognised structural inequities? Mission-specific appropriations don't resolve those inequities by themselves, but they show where a government is willing to hard-wire priorities into the budget.
Targeted appropriations are policy statements in financial form. They show what governments are willing to protect even when competition intensifies elsewhere.
Comparison of Key NIH Grant Mechanisms
| Feature | R01 Research Project Grant | R21 Exploratory/Developmental Grant |
|---|---|---|
| Core purpose | Supports investigator-initiated research programmes with a developed scientific case | Supports exploratory or developmental work where ideas may be earlier-stage or higher-risk |
| Typical policy function | Sustains the main pipeline of established biomedical research | Creates room for concept testing and novel directions |
| Best fit | Researchers with a mature project design and strong rationale | Researchers pursuing less conventional or less fully developed questions |
| Strategic value | Builds continuity and institutional depth | Expands the portfolio's capacity for experimentation |
The wider point is that funding for NIH isn't a single pipeline. It's a toolkit. The strategic question for policymakers is whether that toolkit aligns with the type of science and institutional behaviour they want to encourage.
Currents and Headwinds: Recent NIH Funding Trends and Data
Recent data suggest a more difficult operating environment for NIH applicants and for institutions that depend on NIH-linked research activity. The issue isn't only whether the headline budget looks large. It's whether grantmaking is moving through the system at a pace that supports continuity.
A tighter grantmaking climate
That continuity has weakened. By the end of February FY26, NIH had issued 66% fewer grant awards than the average for the same period in FY21 to FY24, and the dollar value of those awards was 54% lower, according to the Association of American Universities report on the NIH grantmaking slowdown. The same source reported that the 2025 R01-equivalent success rate for early-stage investigators fell from 26% in 2024 to 19% in 2025.
Those figures matter for two reasons. First, they indicate slower throughput, not just tougher competition. Second, they show that early-career researchers face sharper pressure in a constrained environment. A research system can absorb some uncertainty at senior levels. It struggles more when the entry pipeline narrows.
Why this matters beyond US campuses
For international partners, this isn't a narrow workforce issue. It affects the durability of collaborative science. If younger investigators find it harder to secure support, fewer labs gain the autonomy needed to become reliable partners in international consortia. Over time, that can make the ecosystem less diverse, more hierarchical, and more concentrated among already established institutions.
A grantmaking slowdown also changes behaviour before any formal decision arrives. Universities delay hiring. Research centres become more cautious about launching new collaborations. Investigators choose safer projects because they can't afford repeated rejection. None of that needs a dramatic top-line budget cut to become visible.
Here the policy lesson is subtle but important. The health of a research system depends on flow as well as volume. Governments often focus on annual totals because they're politically legible. Scientists and international collaborators live with timing, continuity, and predictability.
- For ministries: slower awards complicate bilateral research planning.
- For universities: uncertainty makes cross-border staffing and trial coordination harder.
- For global health programmes: delayed funding decisions can interrupt work that depends on seasonal, epidemiological, or outbreak-related timing.
That's why short-term turbulence in funding for NIH has consequences that reach beyond the NIH itself.
The Geography of Innovation: Funding Disparities and Global Lessons
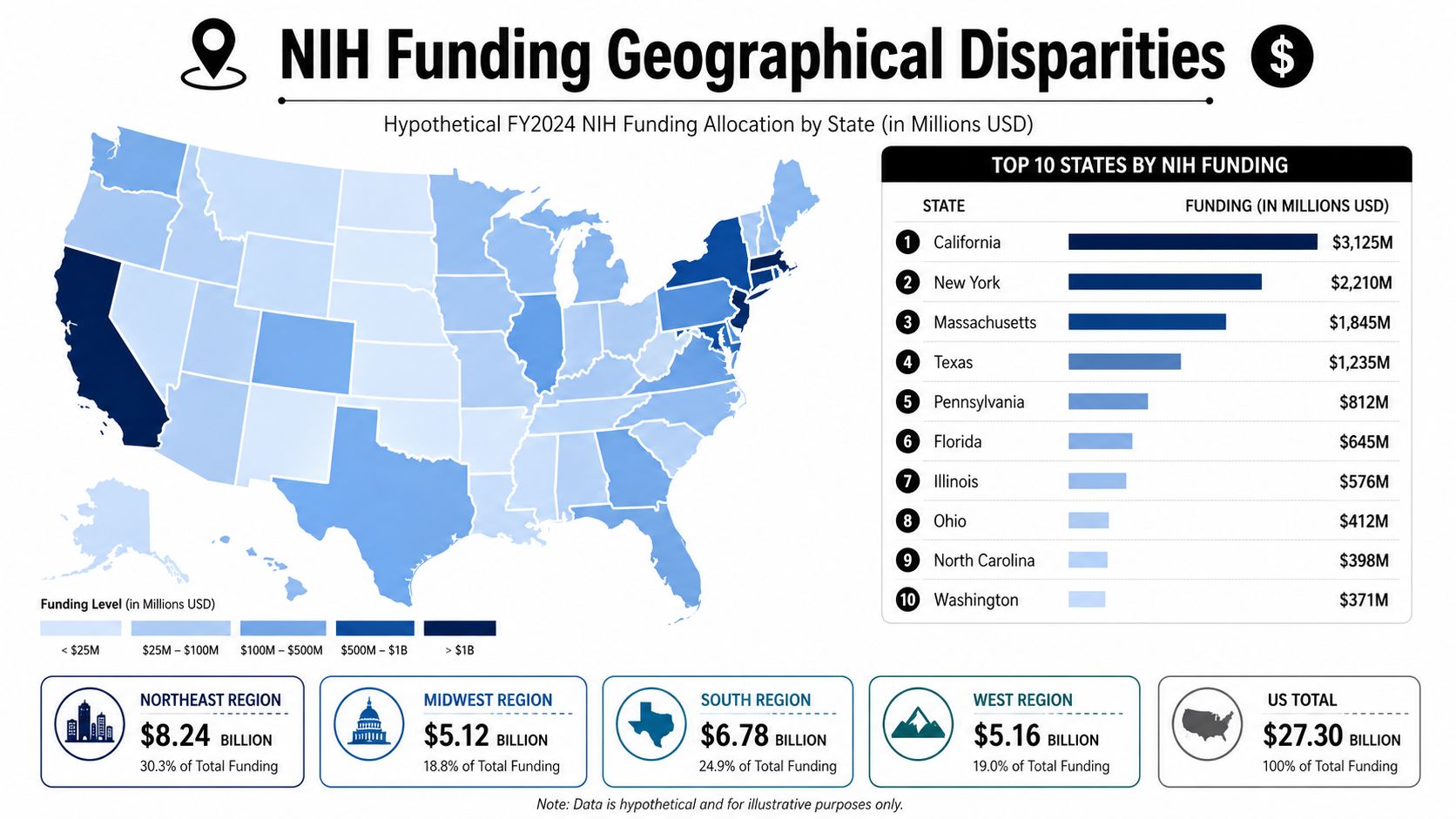
The most neglected question in discussions of funding for NIH is geographical. Not how much the agency spends, but where the benefits accumulate. On that measure, the system looks far less even than the language of open competition suggests.
Concentration is a policy choice
A 2024 study found that non-IDeA states received 93.6% of NIH funding, while IDeA states received 6.4%, even though IDeA states comprise about 46% of US states, according to the Frontiers in Public Health study on the geography of NIH funding. That isn't a small imbalance at the margins. It points to a highly concentrated biomedical map.
The usual defence of concentration is efficiency. Major research hubs have the staff, facilities, patient populations, and administrative depth to use large awards effectively. There's truth in that. High-capacity institutions often produce scale advantages that fragmented systems can't easily match.
But efficiency and access aren't the same thing. A concentrated system may be rational in narrow portfolio terms while still reproducing regional inequality. That matters because capacity doesn't emerge automatically in underserved places. If funding follows existing strength too rigidly, weaker regions remain weaker.
Geographic concentration can produce world-class centres. It can also trap entire regions outside the infrastructure needed to become competitive.
What UK and international funders should learn
The NIH case demonstrates its value for UK and international policy. Many governments now talk about place-based growth, levelling up, regional innovation clusters, and equitable access to public R&D. Yet funding systems often continue to reward already dominant institutions because peer review operates on top of uneven infrastructure.
Three lessons follow.
- Build capacity before demanding equal competition: Regions with thinner research infrastructure need sustained support, not only open calls.
- Measure distribution as well as excellence: Headline outputs can hide deep territorial concentration.
- Use targeted mechanisms deliberately: If a government wants broader regional participation, it needs instruments designed for that purpose.
For the UK, this is directly relevant to debates about whether research spending should deepen existing excellence corridors or seed wider institutional capability. For multilateral institutions, the point is broader. Global health security depends on distributed competence. Outbreak response, population surveillance, and clinical research are weaker when capability is clustered too narrowly.
The NIH experience doesn't prove that concentration is wrong. It shows that concentration has a price. Policymakers should stop pretending that this price is incidental.
Conclusion: Policy Pathways for a Resilient Global R&D Ecosystem
Funding for NIH matters because it combines scale, signalling power, and institutional reach. But the deeper lesson isn't that the United States spends a lot on biomedical research. It's that the structure of that spending creates strategic consequences far beyond US borders.
Three conclusions stand out.
First, stability matters as much as scale. A large budget can still produce insecurity if grantmaking slows, purchasing power erodes, or institutions can't plan across multiple years. Governments that want resilient biomedical ecosystems should prioritise predictable flows, not just politically attractive top-line announcements.
Second, budget architecture is a policy instrument. Mission-specific appropriations, institute-level priorities, and grant mechanisms all shape who can participate and what type of science gets rewarded. International partners shouldn't read NIH as one homogeneous pot. They should read it as a set of strategic choices embedded in administrative design.
Third, geography can't remain an afterthought. The concentration visible in US funding patterns offers a warning to the UK, Europe, and other advanced research systems. Excellence-based competition alone won't correct regional imbalance when institutions begin from very different starting points. If governments care about territorial resilience, they need place-sensitive instruments alongside open competition.
For global health security, that means a stronger multilateral strategy should include at least four moves:
- Track funding volatility early: Foreign ministries, universities, and multilateral agencies should monitor NIH appropriations and award flow as indicators of collaboration risk.
- Invest in administrative capability: Institutions need staff who understand mechanisms, review culture, and institute fit, not just researchers with strong ideas.
- Protect targeted equity missions: Dedicated appropriations can preserve focus on disparities when fiscal conditions tighten.
- Design for distributed capacity: National and international R&D policy should expand the number of places able to host serious biomedical work.
The larger strategic point is straightforward. Biomedical funding is now part of international statecraft. Countries that ignore the mechanics of NIH funding will still feel its effects. Countries that study those mechanics can respond with smarter partnerships, better domestic design, and stronger multilateral resilience.
Global Governance Media brings together policymakers, researchers and international affairs professionals to examine how decisions in one major system reshape global cooperation. If you want more analysis like this on health security, R&D strategy and multilateral policy, explore Global Governance Media.