By Eleanor Markham, Senior Policy Analyst
Health security now depends on information security. Ministers who treat media as a secondary communications issue are missing a growing source of fiscal risk, behavioural volatility, and policy failure.
The strategic problem is no longer limited to illegal content. Governments have built at least partial tools for that task. The harder challenge sits in the space between legality and harm, where inaccurate, sensationalised, or selectively framed health claims can spread at scale without clearly breaching the law. For global governance, the implication is that health risk now travels through two systems at once: clinical systems that manage disease and information systems that shape belief, trust, and compliance.
This is the governance gap G7 and G20 leaders should focus on. A health message can now alter vaccine uptake, mental health help-seeking, emergency response, and institutional credibility before any public authority has time to correct it. The result is more than confusion. It is weaker policy execution, higher social cost, and lower resilience in a crisis.
Global media health should therefore be treated as a policy domain in its own right. It sits at the intersection of public health, platform governance, national security, and democratic legitimacy. The states that perform better will not be those that censor more aggressively. They will be those that build credible rules, faster evidence channels, and trusted public communication systems that can compete in an information market where harmful but legal content often moves faster than verified guidance.
Table of Contents
- The New Frontier of Global Public Health
- Defining the Global Media Health Landscape
- Trends in Health Coverage and Key Media Actors
- How Media Shapes Health Policy and Public Behaviour
- Navigating Misinformation and the Trust Deficit
- Global Media Health in Action Case Studies
- Strategic Recommendations for a Healthier Information Ecosystem
The New Frontier of Global Public Health
Public health ministries still tend to treat media as an instrument for broadcasting decisions already made. That view is outdated. The information ecosystem now shapes whether a health intervention is accepted, doubted, delayed or politically contested before officials can even explain it.
This matters for global governance because health risk now travels through two systems at once. One is biological. The other is informational. Governments can strengthen hospitals, procure medicines and publish guidance, but if citizens encounter conflicting health claims through social platforms, partisan outlets, private messaging groups or creator-led channels, formal policy competes with a faster and often more emotionally compelling stream of interpretation.
Strategic implication: A weak information environment can blunt the value of otherwise sound health policy.
The statecraft challenge is broader than crisis response. In the UK, mental health disorders account for 22.8% of all disease burden, the highest share among health conditions, and anxiety and depression drive 65% of that burden, according to World Health Statistics reporting that draws on UKHSA and NHS Digital analysis. The same source notes that social determinants such as unemployment and housing insecurity increase disorder incidence by 1.4 to 2.1 times per adverse exposure. That means information policy cannot be separated from social policy. Narratives about work, housing, treatment, stigma and institutional competence all affect whether people seek help, delay care or disengage.
For G7 and G20 leaders, the implication isn't just that better messaging is needed. It's that global media health should be treated as part of governance architecture. Countries that fail to manage health information credibly won't just struggle with public understanding. They'll struggle with implementation, legitimacy and cross-border cooperation.
Defining the Global Media Health Landscape
A system, not a channel
Global media health is the interaction between health information, the systems that distribute it, the publics who interpret it and the institutions that respond to its effects. It includes journalism, public service broadcasting, platform algorithms, creator economies, messaging apps, health campaigns, search behaviour and community-level trust networks.
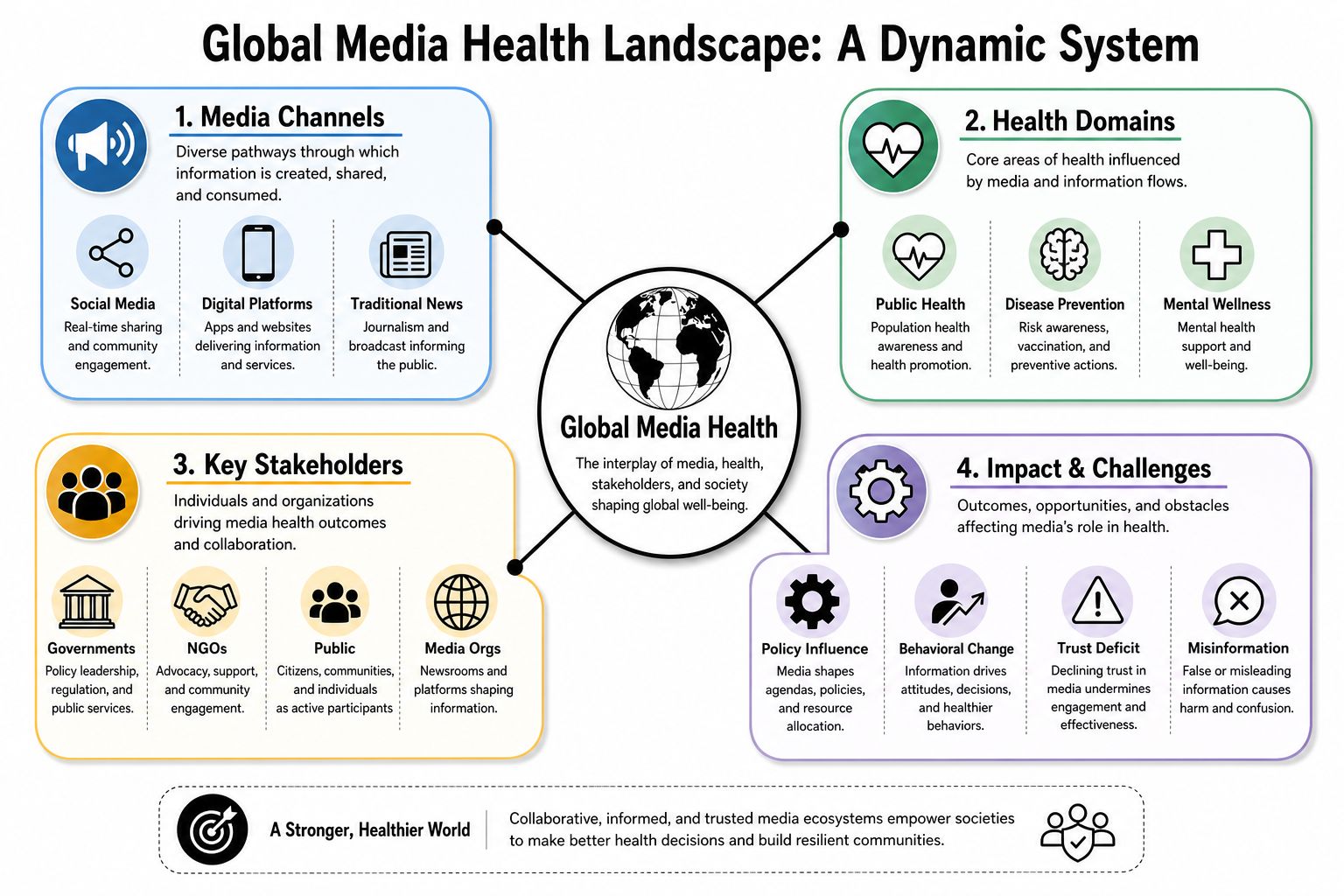
Three components matter most.
- Production and distribution: Newsrooms, ministries, hospitals, NGOs, platforms and influencers all publish health content.
- Reception and interpretation: Audiences don't absorb information passively. They filter it through identity, prior beliefs, community trust and convenience.
- Institutional consequence: Information changes behaviour and shifts the pressure under which ministers, regulators and agencies operate.
That makes the field operational, not academic. A ministry can no longer assume that publishing accurate guidance is enough. It has to consider discoverability, credibility, repetition, translation into everyday language and whether citizens can verify claims across channels.
Why access matters as much as content
One of the most neglected aspects of this field is information inequality. Existing content often highlights the theoretical role of media in raising awareness but fails to provide data-led strategies for overcoming communication inequalities that disadvantage underserved UK populations, especially those affected by the digital divide, as argued in the Health Innovation Yorkshire & Humber digital divide report.
That point deserves ministerial attention. Digital inclusion isn't just a connectivity issue. It's a social determinant of health. If some communities can't reliably access evidence-based health information, compare sources or use digital services, then even strong national guidance can widen inequality in practice.
A useful way to think about the problem is through infrastructure. Roads determine who can reach a hospital. Information systems determine who can reach trusted health knowledge. Both shape outcomes.
For policymakers tracking health in the digital age, the operational lesson is clear. Global media health depends on both content quality and access quality. If one fails, the whole system weakens.
Good policy doesn't only ask whether information is true. It asks who can reach it, who can use it and who is left outside the system.
Trends in Health Coverage and Key Media Actors
Health coverage has become more immediate, more fragmented and more contested. Traditional reporting still matters, especially during acute crises, but it now operates alongside platform-native video, creator commentary, advocacy campaigns and state-backed narratives. As a result, ministers aren't dealing with a single media sphere. They're dealing with overlapping influence systems.
Who shapes the agenda
The strategic challenge is that different actors shape health discourse for different reasons. Some pursue public service. Some pursue engagement. Some aim for geopolitical influence. Others fill trust vacuums left by institutions that communicate too slowly or too technically.
| Actor Type | Primary Channels | Key Characteristics | Impact on Health Discourse |
|---|---|---|---|
| Legacy news organisations | Television, radio, newspapers, websites | Editorial processes, specialist correspondents, agenda-setting power | Can legitimise issues quickly and elevate them into mainstream political debate |
| Digital-native publishers | Websites, newsletters, podcasts, short-form video | Faster production cycles, niche audiences, more interpretive framing | Can shape elite and issue-specific conversations before governments react |
| Social media platforms and creators | Social platforms, video apps, messaging communities | High speed, personal tone, algorithmic amplification, parasocial trust | Can normalise behaviours or doubts rapidly, especially where official voices feel distant |
| State-affiliated media | International broadcasting, digital channels, syndication networks | Strategic framing aligned with national interests | Can internationalise domestic health narratives and politicise scientific questions |
| Public institutions and health agencies | Official websites, campaign assets, press briefings, public information materials | Higher evidentiary expectations, slower approval, formal tone | Can anchor credibility, but may lose reach if content isn't adapted to how people consume information |
Why incentives matter
A minister doesn't need to master every platform dynamic. But they do need to recognise that incentives drive framing. Newsrooms often prioritise conflict, novelty and accountability. Platforms reward retention and reaction. Creators build trust through relatability, not institutional authority. Health agencies prioritise caution and verification. None of those logics are neutral.
That helps explain why accurate information can lose the contest for attention. It also explains why reactive rebuttal is usually too weak. By the time a department corrects a claim, audiences may already have absorbed a more vivid version from a source they feel they know personally.
Policymakers following debates about how AI helps YouTube health transform the reach and scale of high-quality health information should treat technology as an amplifier, not a substitute for institutional strategy. AI can improve distribution and discovery, but it can't repair weak trust or unclear accountability on its own.
The decisive question isn't who publishes first. It's who becomes the public's default interpreter of uncertainty.
How Media Shapes Health Policy and Public Behaviour
Media now functions as part of health system performance. It influences risk perception, treatment choices, social norms and the political timetable for intervention. For G7 and G20 governments, that makes the information environment a governance issue, not a communications side question.
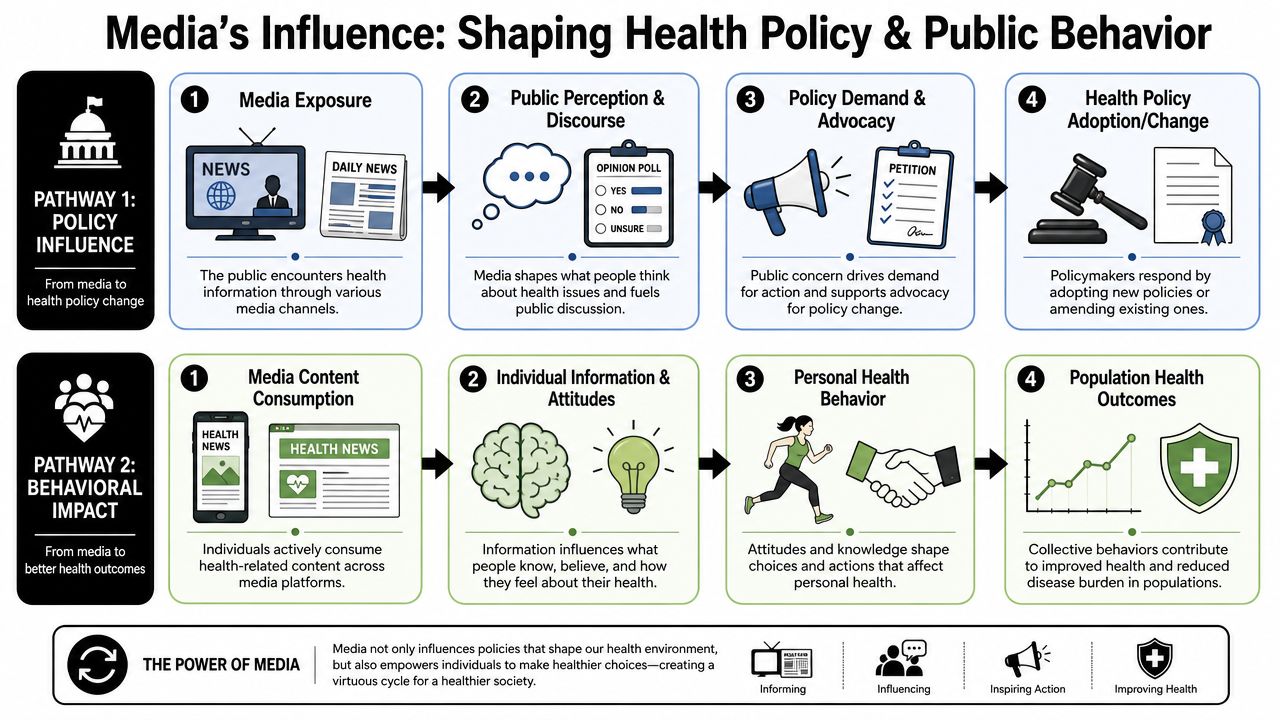
The behavioural pathway
Adolescents provide one of the clearest signals. Problematic social media use among adolescents in the WHO Regional Office for Europe rose from 7% in 2018 to 11% in 2022, with girls reporting 13% and boys 9%, according to WHO Europe reporting on teens, screens and mental health. The same source reports that 12% of adolescents are at risk of problematic gaming. It also notes that a forthcoming 2026 academic study is expected to examine whether very high daily social media use among fifteen-year-old girls in the UK is associated with lower life satisfaction.
The policy implication is broader than screen-time anxiety. Media exposure helps shape sleep routines, self-image, stigma, perceived peer behaviour and thresholds for seeking help. Those effects accumulate through repetition and social reinforcement, not only through explicit persuasion.
Health behaviour follows a chain. People first notice an issue, then decide whether it applies to them, then judge whether action feels normal, feasible and worth the effort. Media can alter each stage. A news cycle can raise salience. Creator content can redefine what counts as credible advice. Repeated anecdote can outweigh formal guidance if it feels more immediate or more personally relevant.
That is why governments need a wider frame than content accuracy alone. The strategic challenge is influence architecture, who sets norms, who interprets uncertainty, and who benefits when confusion persists. Our analysis of health disinformation as a governance and democratic resilience challenge sets out why this extends beyond public health into state capacity.
The policy pathway
Media also shapes what becomes governable. Sustained coverage can compress decision timelines, trigger parliamentary scrutiny, shift regulator attention and raise the political cost of delay. Limited coverage can produce the opposite outcome. A material health risk may remain visible to specialists yet fail to attract the authority or budget needed for response.
Ministers should therefore treat media conditions as part of policy design. If implementation depends on trust, uptake or coordinated behaviour across agencies, then the communication environment affects delivery in the same way as workforce capacity, procurement or local infrastructure.
A practical framework for ministers is straightforward:
- Track exposure patterns: Monitor where specific populations encounter health claims, advice and commentary.
- Map trusted intermediaries: Identify which clinicians, creators, community leaders and institutions carry persuasive authority with different groups.
- Test behavioural friction: Examine why guidance fails at the point of action, including confusion, stigma, low convenience or contradictory signals.
- Prepare agenda scenarios: Plan for periods of intense coverage, partial coverage and hostile framing, then align response capacity to each case.
The reason is that public behaviour does not move only through evidence. It moves through evidence filtered by narrative, trust and social proof. That is also why crisis planning should include protocols for addressing misinformation in health crises before the next controversy forces decisions under pressure.
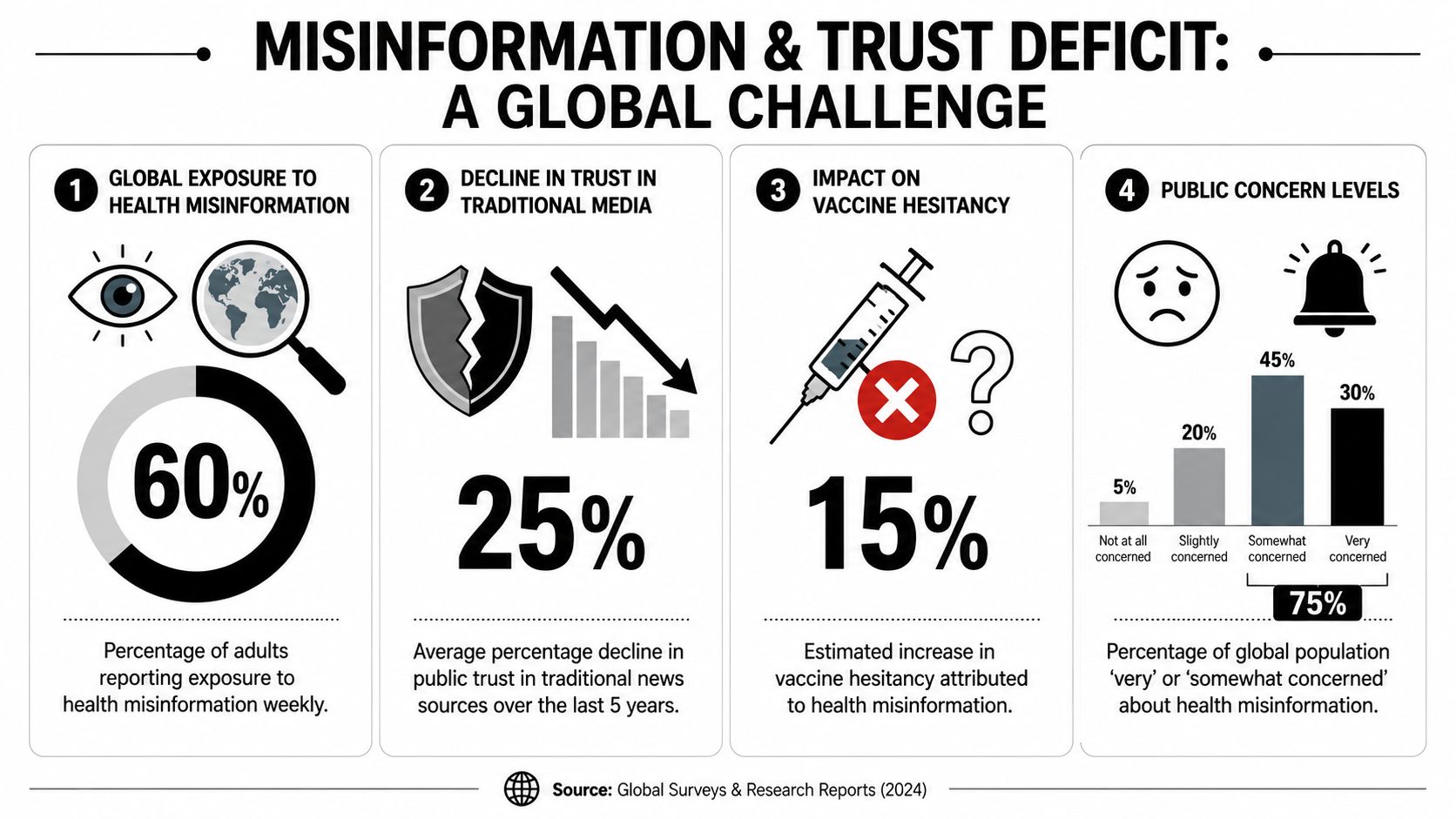
Navigating Misinformation and the Trust Deficit
The hardest policy problem in global media health isn't illegal content. It's lawful content that still causes public harm. Much of the current debate collapses these categories, which leads to weak regulatory design and confused enforcement.
The legal gap policymakers underestimate
Recent UK-focused analysis identifies a policy gap between regulating illegal content and mitigating harmful but legal misinformation in medicine. It argues that existing coverage often conflates the two and that there's insufficient clarity on how platforms should be guided to address dangerous non-illegal health claims, leaving a practical enforcement vacuum for policymakers, as set out in this analysis on tackling misinformation in UK medicine.
This distinction matters because many harmful claims don't cross a legal threshold. They may be selectively framed, misleading by omission, dressed in scientific language or spread through anecdote rather than explicit falsehood. That makes them harder to regulate and easier to defend.
A government that responds only through takedown powers will miss the larger threat. The primary governance challenge is establishing rules, incentives and public expectations for content that remains lawful yet corrodes health decision-making.
Trust is the strategic asset
The downstream effect isn't merely confusion. It's erosion of trust in medicine, regulators and democratic institutions. Once citizens conclude that every health claim is political, every expert compromised and every platform arbitrary, the state loses authority precisely when it needs collective action.
That is why operational guidance matters during fast-moving emergencies. Resources on addressing misinformation in health crises are useful not because they promise a silver bullet, but because they emphasise speed, clarity and messenger discipline during periods when rumours can outpace formal communication.
For policymakers concerned with health in the age of disinformation, protecting truth and protecting democracy, the strategic test is whether institutions can reduce harm without undermining legitimate debate. That requires better standards for evidence, provenance and accountability, not just louder rebuttals.
- Differentiate categories: Illegal deception, dangerous misinformation and good-faith disagreement require different responses.
- Build verification habits: Schools, public campaigns and health systems should normalise source-checking as routine behaviour.
- Set platform expectations: Governments should define what procedural responsibility looks like even where removal isn't warranted.
Global Media Health in Action Case Studies
Global media health is now a governance issue, not a communications side topic. Recent case studies show that the hardest policy failures rarely come from clearly illegal content alone. They arise in the wider zone of harmful but lawful claims, weak institutional signalling and delayed public response.
Pandemic communication
Covid-19 exposed a simple fact. Health emergency management and information management are inseparable. Governments that treated communication as a downstream function of policy often lost control of the public narrative, even when the underlying science was sound.
Daily briefings, dashboards and televised announcements gave states unusual reach into everyday decision-making. Yet reach did not guarantee compliance or trust. Where guidance changed without clear explanation of what evidence had shifted, many citizens read revision as incompetence, political pressure or concealment. In practice, the policy problem was not only what governments said. It was whether institutions had prepared the public to expect uncertainty, changing baselines and incomplete knowledge in a fast-moving crisis.
The strategic lesson is clear. Crisis communication systems should be designed to explain why advice changes, who is accountable for updates and what remains uncertain. Ministers need a standing capability for this before the next emergency, not an improvised press operation once confusion is already widespread.
Vaccines and narrative fragility
Vaccination campaigns demonstrate how quickly health policy can be weakened by narrative instability. Supply chains, procurement and distribution matter. So does the perceived legitimacy of the programme itself.
Once vaccine debate is framed through identity, grievance or distrust of institutions, factual rebuttal becomes less effective on its own. A relatively small volume of repeated doubt can alter media agendas, slow uptake in hesitant communities and force governments into reactive politics. That governance burden matters. It diverts administrative attention, raises delivery costs and widens the gap between national policy design and local public response.
This is the core policy challenge that current regulation only partially addresses. Much of the content that undermines vaccine confidence is not illegal. It sits in the category of harmful but legal speech, where the state has fewer direct tools and platforms often face weak procedural expectations. For G7 and G20 leaders, that gap should be treated as a strategic risk to health security.
Operational lesson: Build rebuttal capacity, community partnerships and local messenger networks before controversy peaks.
Mental health coverage
Mental health presents a different test. Here, media exposure can produce public benefit and public harm at the same time.
Good coverage can reduce stigma, widen recognition of symptoms and make help-seeking more socially acceptable. Poor coverage can compress serious disorders into lifestyle language, reward self-diagnosis and blur the distinction between temporary distress and clinically significant illness. That distortion has direct policy consequences. It can increase demand for poorly matched services, confuse public expectations about treatment and weaken shared understanding of severity and evidence.
As noted earlier, the economic and workforce costs associated with poor mental health are already substantial. Ministers therefore have a clear interest in the quality of mental health narratives across broadcast, print and digital platforms, not only in the availability of services.
Three lessons stand out:
- Link awareness to care pathways: Public attention is useful only when audiences can identify credible routes to assessment, treatment and support.
- Use trusted intermediaries: Teachers, employers, community leaders and frontline health workers often interpret mental health information more effectively than central campaigns.
- Protect clinical clarity: Stigma reduction should not come at the cost of precision about diagnosis, severity and evidence-based treatment.
Strategic Recommendations for a Healthier Information Ecosystem
G7 and G20 leaders need a governance response equal to the scale of the problem. The aim isn't to control debate. It's to create conditions in which evidence-based health information can compete fairly, reach broadly and retain public trust.
What ministers should do now
Make infodemic management a core public capability. Health ministries should build standing teams that combine policy, behavioural insight, digital monitoring and rapid-response communications.
Create a distinct policy category for harmful but legal health misinformation. Regulators need clearer frameworks for transparency, labelling, amplification standards and platform duties where outright illegality isn't the issue.
Adopt evidence standards for public-facing health content. The NHS has already set a useful benchmark through six core principles for clinical information, including the requirement that content use "relevant, up to date and recognised clinical evidence", with Principle 2 explicitly requiring reliance on verified clinical data, as outlined in the NHS standard for creating health content.
Treat digital inclusion as health policy. If vulnerable groups can't access trustworthy information, information inequality will continue to deepen outcome inequality.
Build cross-border norms through the G7 and G20. Shared expectations on platform responsibility, health information provenance and emergency communication practice would improve coordination during future crises.
Require accountability in promotional health claims. UK pharmaceutical advertising rules under the ABPI Code require promotional materials to be certified by appropriately qualified persons before use and recorded accordingly, as summarised in the UK guide to medicines and medical devices advertising rules. That principle of named responsibility is worth extending more broadly across high-risk health communications.
The central point is simple. Governments can't protect public health if they ignore the health of the information environment.
Global challenges need institutions that can turn complexity into action. Global Governance Media gives policymakers, officials and international leaders a place to track emerging risks, test strategic ideas and engage with evidence-led analysis on the issues shaping the G7 and G20 agenda.