By Dr Eleanor Hart, Senior Health Policy Analyst
The most counterintuitive fact about public private partnerships in healthcare is that their biggest policy risk often appears after the ribbon-cutting, not before it. In the UK, the National Audit Office found that the Private Finance Initiative had delivered 127 NHS hospitals and 3,369 other public buildings by March 2018, yet it also tied the public sector into typically 25–30 year unitary-payment contracts while transferring only limited risk away from the state, as summarised in this review of UK PFI experience. That finding should change how ministers think about partnerships. A facility can be delivered faster and still leave the state with inflexible liabilities, weak influence over performance, and little room to redesign services later.
That is why the current debate needs a reset. Across G20 health systems, fiscal pressure, ageing populations, workforce shortages, digitisation demands, and uneven territorial access are all pushing governments back towards partnership models. But the old infrastructure-first lens is no longer enough. The central policy question isn't whether governments should work with private actors. They already do. The core question is whether they can govern those relationships in ways that protect affordability, improve equity, and preserve public legitimacy.
Table of Contents
- The Renewed Imperative for Healthcare Partnerships
- Decoding the Spectrum of Healthcare PPP Models
- Financing Structures and Long-Term Contractual Risks
- Designing Robust Governance and Risk Allocation
- Evaluating Performance Beyond Project Completion
- The Next Frontier Digital Health and Data Partnerships
- Actionable Policy Recommendations for 2026 and Beyond
The Renewed Imperative for Healthcare Partnerships
Healthcare partnerships are back on ministerial agendas because public systems need capacity, speed, and technical capability. But many earlier arrangements underperformed not because partnership was the wrong idea, but because governments treated it as a financing shortcut rather than a governance discipline.
The pressure is now broader than hospital construction. Health ministries need interoperable records, analytics capacity, community-based service redesign, resilient supply chains, and operating models that can reach underserved populations. Those needs often exceed what public agencies can build quickly on their own. Yet private participation only creates public value when the state remains an intelligent purchaser, regulator, and steward.
A practical implication for G20 governments is that public private partnerships healthcare should be framed as a strategic capability choice, not a budgetary workaround. In federal and complex public systems, implementation often depends on dependable technology and delivery partners who understand public sector operating constraints. For officials examining that execution layer, the discussion around the RiverAxe health IT partnership is useful because it reflects the kind of specialised vendor alignment public agencies increasingly need when digital infrastructure and service continuity matter.
The shift ministers should recognise
Traditional debates have focused on ownership and ideology. That framing is now too crude. The sharper policy divide is between partnerships designed around procurement mechanics and partnerships designed around outcomes.
Practical rule: If a partnership's success criteria stop at asset delivery, ministers should assume that the hardest public-interest questions haven't yet been addressed.
Health leaders also need a wider lens on system priorities. The broader case for sustainable public health strategy is well reflected in this analysis on prioritising global healthcare, which places financing, resilience, and access in the same policy frame. That is the correct frame for partnership decisions as well.
Decoding the Spectrum of Healthcare PPP Models
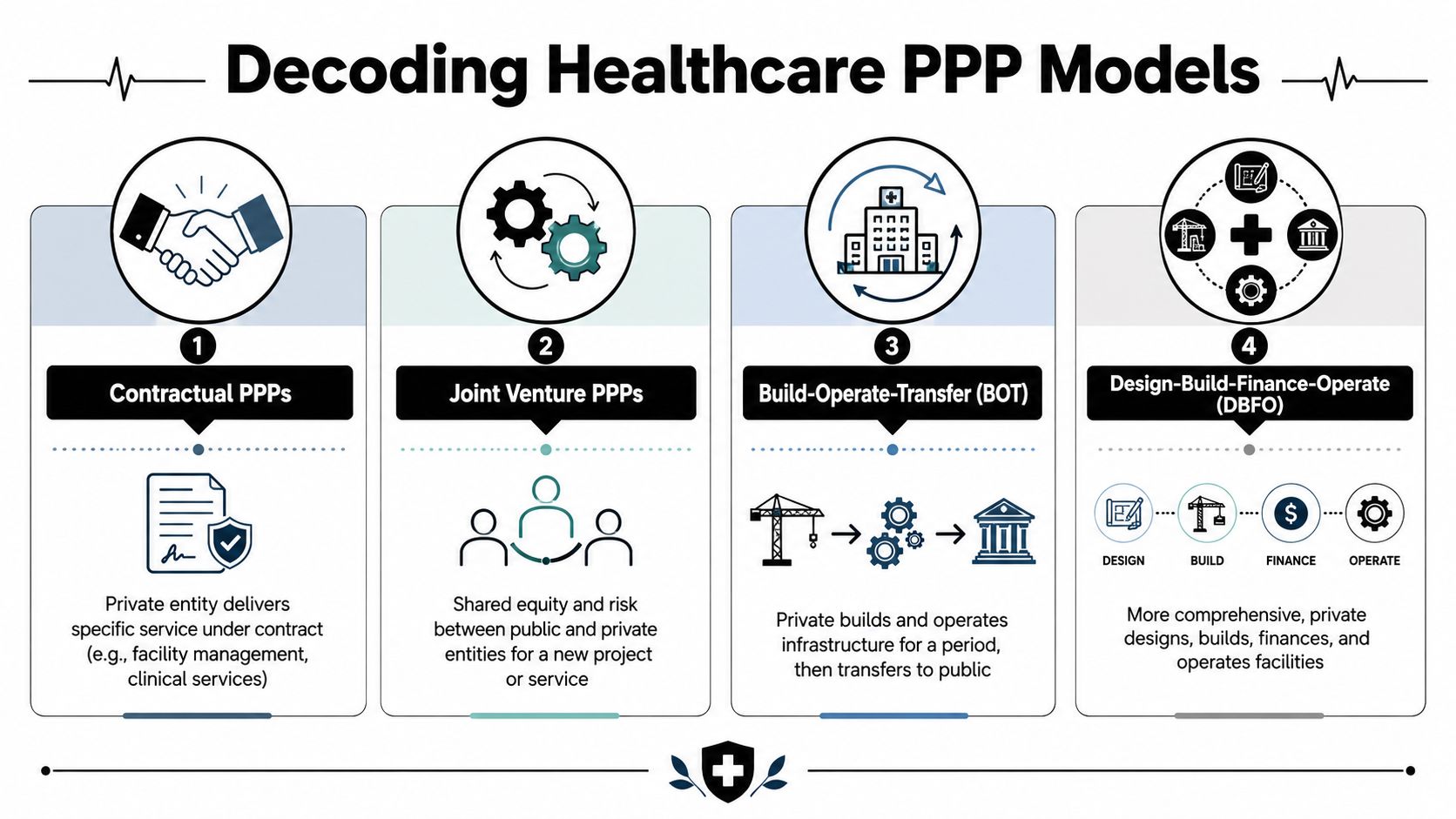
Not all healthcare PPPs do the same job. Some procure a building. Some outsource a service. Others create a long-term joint operating arrangement. The model determines who pays, who manages, who can adapt the service, and who bears failure when assumptions prove wrong.
Why model choice matters
A contractual PPP is often the simplest form. The public sector retains strategic control and pays a private provider to deliver a defined service such as facilities management, diagnostics support, or a digital platform. This can work when outputs are clear and switching costs are manageable.
A joint venture PPP goes further. Public and private partners share ownership, governance, and risk in a new entity or programme. This model can support innovation, but it also complicates accountability because commercial and public-service logics sit inside the same structure.
A Build-Operate-Transfer arrangement usually centres on infrastructure. The private partner builds and operates the asset for a defined period before transfer. This model can speed delivery, but ministers need to ask whether service design may need to change before transfer occurs.
A Design-Build-Finance-Operate model is the most complete. The private party handles the full lifecycle from design through operation. It can align incentives across stages, but it also creates long-term lock-in if contracts are rigid or demand assumptions prove unrealistic.
Comparison of common healthcare PPP models
| Model | Private Sector Role | Primary Public Sector Payment | Key Risk Transferred to Private Sector |
|---|---|---|---|
| Contractual PPP | Delivers a specific service under contract | Service fees or availability-based payments | Service delivery and operational performance within contract scope |
| Joint venture PPP | Shares ownership and operational responsibility | Capital contribution, service purchasing, or mixed financing | Shared commercial and execution risk |
| Build-Operate-Transfer | Builds and runs infrastructure for a fixed term | Availability payments, usage payments, or hybrid arrangements | Construction and early operational risk |
| Design-Build-Finance-Operate | Designs, builds, finances, and operates facility or service platform | Long-term unitary or availability-style payments | Design, construction, financing, and operational integration risk |
The policy mistake is to ask which model is best in the abstract. The right question is narrower. Which model matches the asset or service, the state's oversight capacity, the need for flexibility, and the intended population outcome?
The control question often missed
Governments often assume that more risk transfer means a better deal. It doesn't. Some risks can be transferred contractually, but strategic accountability for patient care, continuity of service, and equity remains public. If ministries can't monitor quality, verify data, or enforce corrective action, formal risk transfer may have little practical meaning.
For policymakers interested in partnership design beyond theory, this reflection on enabling partnerships to drive the future of health usefully captures the move from broad collaboration rhetoric to delivery-oriented institutional design.
Financing Structures and Long-Term Contractual Risks
A healthcare PPP can stabilize delivery or hardwire fiscal stress for a generation. The difference usually sits in the payment formula, the refinancing terms, and the contract's ability to absorb service change.
What unitary payments really mean
In long-term healthcare PPPs, the public authority often commits to a single periodic payment that covers capital recovery, facilities management, maintenance, financing costs, and sometimes selected non-clinical services. That structure can make annual budgeting more predictable. It can also narrow strategic room to act if clinical models shift, hospitals need repurposing, or policymakers want to move care into primary, community, or home-based settings.
This matters more in health than in transport or energy.
A hospital, diagnostic network, or digital service platform is not a static asset. It sits inside a delivery system shaped by demographic change, new treatment pathways, workforce shortages, and data-driven care models. A financing structure that appears affordable at financial close can become poor value if variation charges are high, output specifications are too rigid, or payment deductions are too weak to change provider behavior.
The practical test is not whether private finance accelerated delivery. It is whether the state preserved enough freedom to redesign services without paying heavily for each adjustment.
Why long contracts create hidden policy exposure
The main fiscal risk in healthcare PPPs is often not the initial capital cost. It is the accumulation of fixed payment obligations against an uncertain service model. Ministries of health may sign contracts on the basis of current bed numbers, current referral patterns, or current administrative processes, then discover a decade later that the contract rewards asset utilization rather than system efficiency.
That problem is now sharper in digital health. G20 governments are no longer contracting only for buildings and equipment. They are increasingly procuring interoperable records, diagnostics platforms, telehealth infrastructure, cybersecurity services, and data hosting arrangements. Those assets depreciate faster, standards evolve more quickly, and vendor dependence can grow through proprietary architecture rather than concrete and steel. In these cases, a long contract can create technology lock-in as well as fiscal lock-in.
For data-sharing and digital service partnerships, privacy compliance should be priced and monitored from the start, not treated as a legal annex added late in procurement. For a practical reference on governance expectations in regulated environments, see mandatory privacy assessments for Alberta businesses.
The policy lesson from UK PFI
The UK record remains instructive because it shows how a financing solution can outlast the assumptions that justified it. Reviews by the UK National Audit Office found that private finance deals often provided infrastructure on time, but public bodies remained tied to long payment streams and faced high costs when they needed to alter buildings or service specifications, as set out in the National Audit Office review of PFI and PF2.
The lesson for G20 ministers is specific. Long-term commitments should be judged against health-system adaptability, not procurement completion. A contract can succeed on construction metrics and still impede later reforms in prevention, integrated care, digitization, or geographic equity.
Three financing questions deserve ministerial attention before tender:
- How does affordability perform under different care models? Test the payment profile against scenarios such as lower inpatient demand, greater outpatient substitution, or expanded digital monitoring.
- Which risks are effectively transferred, and which return through renegotiation? Refinancing gains, force majeure treatment, demand shifts, and contract variations often reveal whether the public side still carries the harder risks.
- What is the cost of changing course? Price the likely need to reconfigure wards, add digital functions, revise data requirements, or rebalance services toward underserved populations.
What disciplined finance governance looks like
Sound finance governance starts with joint appraisal by health, finance, and digital authorities, not with a procurement exercise led by infrastructure teams alone. The central question is whether the state is paying a premium for private capital without securing corresponding gains in execution, maintenance discipline, service quality, or innovation capacity.
Contracts should therefore include clear breakpoints for review, transparent refinancing rules, and mechanisms for technology refresh where digital components are material. They should also distinguish between assets that benefit from long amortization periods and digital systems that may need shorter cycles, modular procurement, or staged competition.
The wider policy implication is straightforward. Financing choices in healthcare PPPs shape future policy space. Governments that want partnerships to advance equity and digital transformation, not just build facilities, need contracts that preserve flexibility where the health system is most likely to change.
Designing Robust Governance and Risk Allocation
Contracts don't govern themselves. Even well-drafted agreements drift if the public authority lacks people, data, and escalation channels to manage performance over time. In public private partnerships healthcare, governance quality often matters more than procurement sophistication.
Governance must outlast procurement
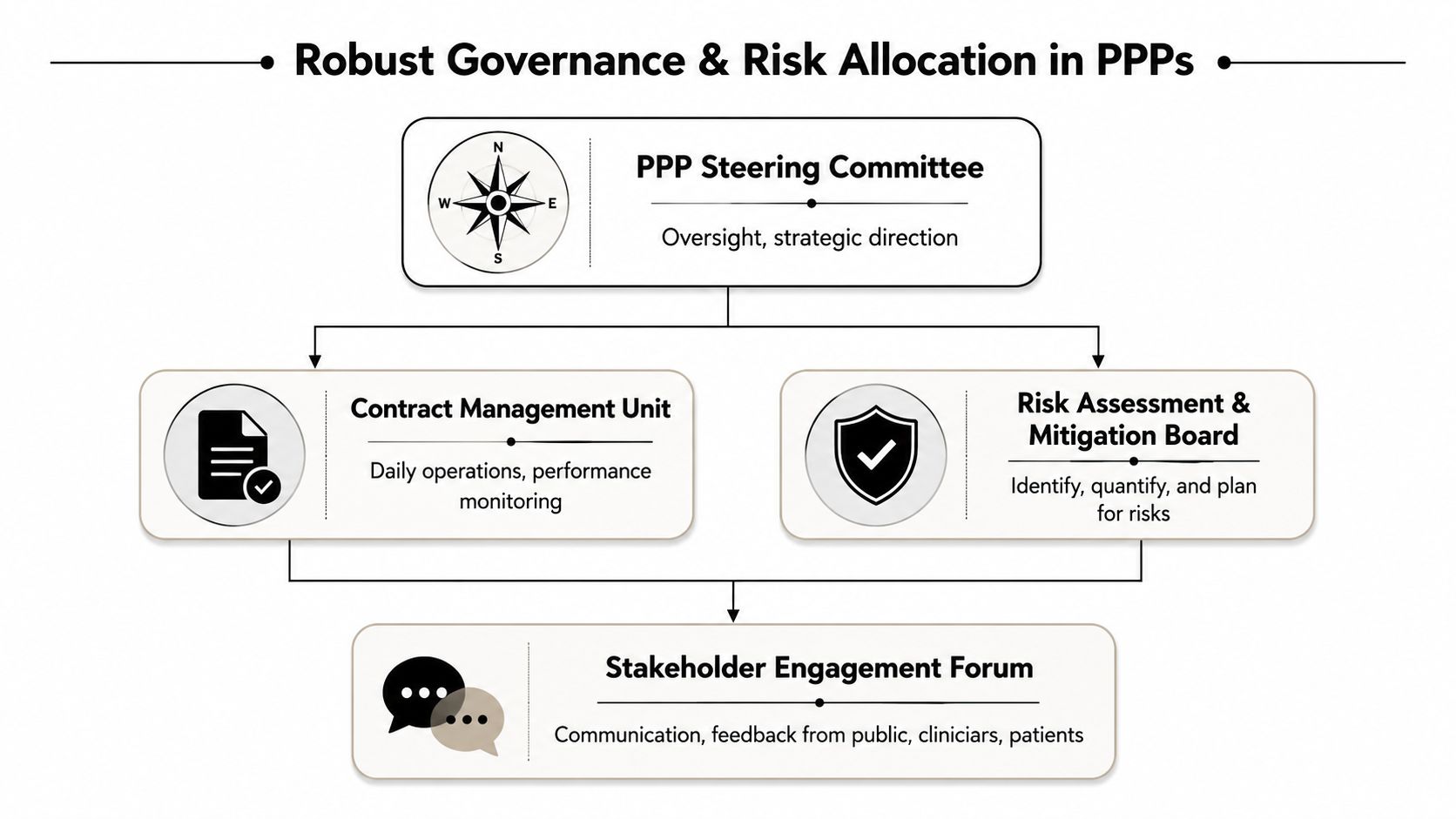
A strong governance architecture usually includes a steering body with decision authority, a contract management unit that understands both operational and financial terms, and an independent assurance function able to review disputes, performance claims, and compliance issues. Without those elements, public agencies tend to manage by exception and respond only when problems become visible to ministers or the media.
Healthcare adds another layer. Clinical quality, patient safety, access, and continuity of care cannot be reduced to generic vendor management. The public side needs governance that combines legal, financial, technical, and service expertise.
A modern governance framework should include:
- Dedicated contract management: not an ad hoc team assembled after signature, but a standing capability with operational authority.
- Independent monitoring: someone outside day-to-day delivery must be able to validate reported performance and challenge selective data.
- Clear dispute pathways: unresolved ambiguities become hidden costs if no structured escalation route exists.
- Stakeholder voice: clinicians, patients, and local authorities need formal channels into review processes.
Which risks can move and which cannot
Some risks can be assigned meaningfully to the private party. Construction delays, build defects, or specified operational failures often fit that category. But other risks remain public even if the contract says otherwise. Governments still carry ultimate responsibility for patient care, system continuity, and political accountability when services fail.
The state can contract out tasks. It can't contract out stewardship.
Digital partnerships make this even more demanding. Data misuse, weak interoperability, and poor consent practices can destroy trust quickly. For officials dealing with privacy and compliance design, practical frameworks such as these mandatory privacy assessments for Alberta businesses are useful reference points because they illustrate the discipline required before sensitive data systems go live.
The core governance test is simple. If the public authority cannot observe performance clearly, intervene lawfully, and explain decisions transparently, the partnership is under-governed.
Evaluating Performance Beyond Project Completion
Too many PPP scorecards stop at delivery. Was the facility built. Was the platform launched. Did the supplier meet the contractual milestone. Those questions matter, but they don't tell ministers whether public value was created.
Access is not the same as equity
One of the most under-answered questions in the UK context is whether healthcare PPPs improve access in underserved geographies once travel, staffing, and digital exclusion are taken into account, not merely when a facility exists. A review of healthcare PPP research notes that the evidence base remains largely descriptive and focuses more on access, prevention, and treatment projects than on hard equity outcomes, while also stressing that trust, data-sharing, mutual value creation, and accountability are central enablers in successful partnerships, as discussed in this review of healthcare PPPs and equity-related implementation issues.
That point has broad G20 relevance. A partnership can increase nominal service capacity and still leave rural communities, coastal populations, deprived districts, or digitally excluded households behind. If ministers don't measure those gaps, they may overstate success.
What ministers should measure instead
A stronger evaluation frame should combine operational metrics with public-interest outcomes. That means asking not only whether the service runs, but who can use it, who trusts it, and who still faces barriers.
A practical monitoring set might include:
- Geographic reach: whether the service reduces practical distance and travel burdens for priority communities.
- Workforce usability: whether staffing models support sustained delivery instead of creating fragile dependence on external provision.
- Digital inclusion: whether online pathways are usable for people with low connectivity, low digital confidence, or language barriers.
- Community trust: whether patients and local clinicians believe the arrangement is accountable and responsive.
- Adaptation capacity: whether the partnership can change as population needs change.
If a partnership improves throughput for already-served populations but leaves excluded groups untouched, it hasn't solved the policy problem that justified it.
Procurement-centred governance fails. Contracts usually specify outputs. Equity requires ministries to specify distributional outcomes, review them regularly, and act when they diverge from intention.
The Next Frontier Digital Health and Data Partnerships
The centre of gravity in healthcare PPPs is shifting away from buildings alone. Partnerships increasingly involve telehealth, analytics, shared data environments, digital triage, AI-supported workflow tools, and population health platforms.
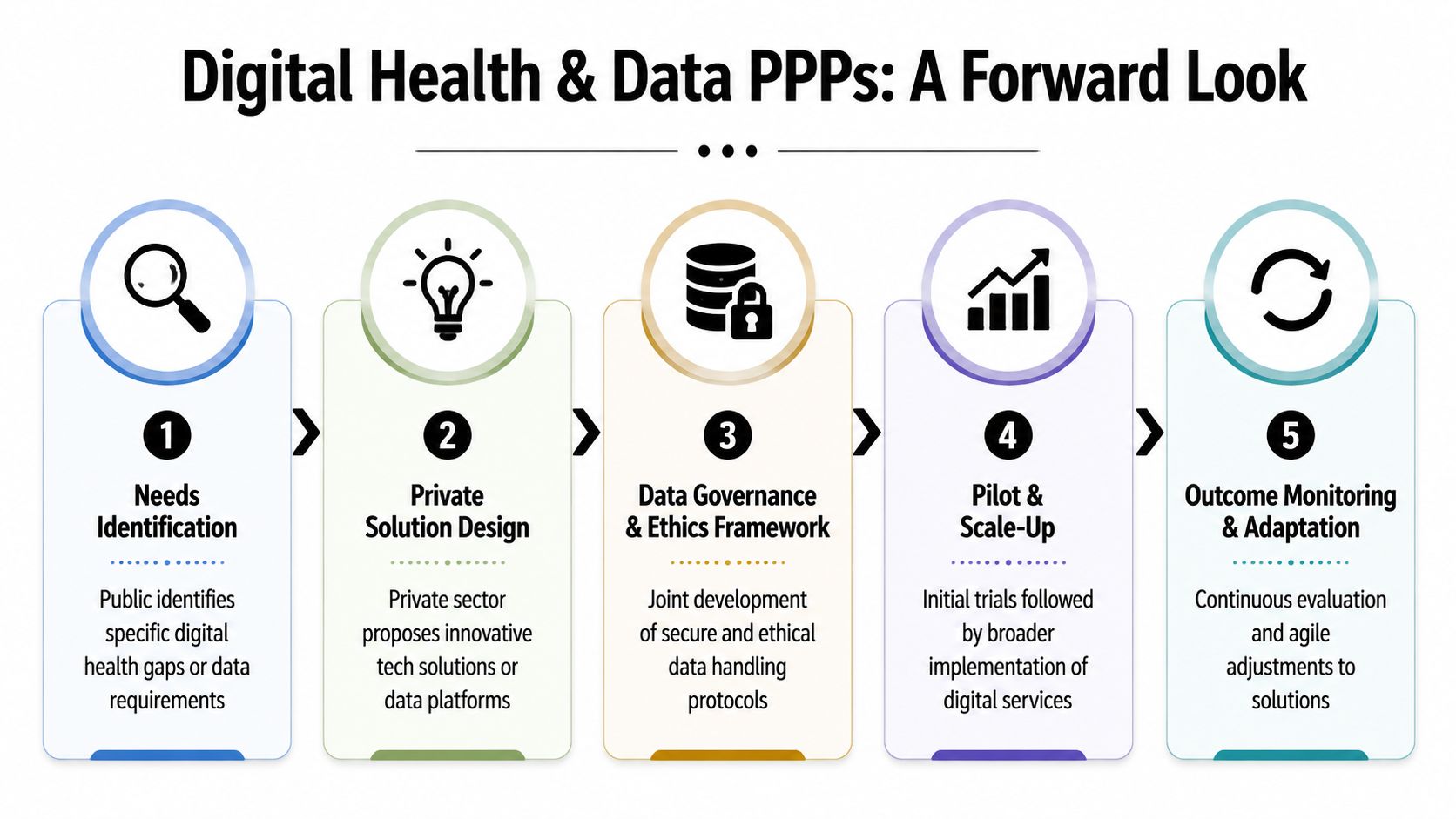
From buildings to digital operating models
A recent review argues that healthcare PPPs increasingly apply across the continuum of care and require analytics, AI, and bidirectional information flow to work well. It also notes that this changes the debate from hospitals and equipment to digital operations and data governance, while raising practical questions about digitisation, interoperability, and local service redesign, as examined in this 2023 review of healthcare PPPs and digital service models.
That is a major policy shift. In digital PPPs, the core asset may not be a building at all. It may be a workflow engine, a referral management system, a shared data layer, or an AI-supported patient access tool. Governments therefore need contracts that govern data rights, model oversight, interoperability duties, audit access, and service continuity.
A broader policy discussion on digital health is useful here because it captures the extent to which digital capacity is now inseparable from health-system performance.
Later in the section, this short briefing adds context on how digital transformation is changing healthcare delivery:
Data governance becomes the core contract
The usual PPP question used to be, who owns and maintains the asset. The digital-era question is different. Who controls the data, who can access it, who validates algorithmic outputs, and who is accountable when automated systems disadvantage specific populations?
These are not side issues. They are the contract.
For policymakers looking at practical examples of AI-enabled patient operations, the account of how GI Partners uses AI is useful because it shows how quickly private capability is moving into frontline access workflows. That creates opportunity, but it also means public buyers must ask harder questions about explainability, fairness, escalation, and human override.
Digital partnerships should therefore include several essential elements:
- Interoperability obligations: vendors must work within public architecture, not trap agencies in proprietary dead ends.
- Audit rights: ministries need access to performance evidence, model behaviour records, and incident logs.
- Data minimisation and purpose control: partners shouldn't use public health data beyond the agreed public purpose.
- Exit planning: the state must be able to switch provider or bring capability in-house without service collapse.
The next frontier is not more technology for its own sake. It is a public governance model capable of using private innovation without surrendering public accountability.
Actionable Policy Recommendations for 2026 and Beyond
The policy test for healthcare PPPs has changed. By 2026, the central question is whether governments can use private finance, delivery capacity, and digital innovation without weakening public control over equity, data, and service continuity.

Priorities for multilateral actors
G20 institutions, development banks, and global health agencies should define a clearer international baseline for healthcare PPP quality. The priority is not a single model contract. It is a shared framework for testing fiscal value, publishing contract terms, measuring distributional effects, and setting rules for digital infrastructure, data access, and vendor accountability.
They should also shift technical assistance away from deal origination alone and toward long-term state capability. Many ministries can reach financial close. Far fewer can supervise performance, renegotiate terms without losing public value, or intervene when digital vendors control data flows that shape access and clinical operations. Peer learning should therefore focus on contract management units, data governance capacity, and methods for tracking whether partnerships improve access for underserved populations.
A practical implication follows. Multilateral support should reward governments that build oversight systems before scaling PPP pipelines.
Priorities for national governments
Health and finance ministries should apply a tougher entry filter. A partnership should proceed only when it solves a defined system problem better than direct public provision, conventional procurement, or targeted service contracting.
Five actions matter most:
- Approve only where the state has governing capacity: if the purchaser cannot monitor service standards, enforce penalties, and manage disputes, private participation increases risk rather than reducing it.
- Require equity testing at appraisal and during delivery: each major PPP should be assessed for its effects on rural access, low-income patients, disability inclusion, and digital exclusion, with corrective triggers written into the contract.
- Use revision clauses tied to public need: health demand, clinical pathways, and technology change faster than most long-term agreements. Contracts should allow service redesign without excessive renegotiation costs.
- Treat digital governance as core contract design: interoperability, cybersecurity duties, audit access, data-use limits, and human oversight of algorithmic tools should sit in the main body of the agreement.
- Judge performance on public outcomes after launch: governments should review waiting times, continuity of care, trust, resilience under stress, and fairness in access, not only whether an asset was delivered on time.
The wider lesson is strategic. The next generation of public private partnerships healthcare should be assessed less by the volume of private capital mobilised and more by whether public authorities retain the ability to set terms, inspect results, and correct course when partnerships drift away from national health goals.
For more policy analysis on global health, digital governance, and G20 decision-making, explore Global Governance Media, where leaders and practitioners can follow practical, evidence-based perspectives on the choices shaping public systems.