


By Global Governance Media Analysis Desk
More than 2.5 million patients served worldwide is the figure that most clearly reframes the AIDS Healthcare Foundation for a policy audience. At that scale, AHF is no longer best understood as a single NGO or advocacy brand. It is a transnational delivery platform, a political actor, and a test case for how large civil society organisations can shape international health governance through service provision as much as through campaigning.
For G7 and G20 delegates, that matters because HIV governance increasingly turns on execution rather than declaration. Countries don't just need commitments on prevention, testing, treatment, and linkage to care. They need institutions that can sustain those functions across different regulatory and financing environments. AHF's model raises a sharper question than most commentary admits. When a nonprofit reaches global scale, how should governments engage it: as a partner, a contractor, an advocate, a competitor, or all four at once?
Table of Contents
- The AIDS Healthcare Foundation in Global Health
- Origins and Organisational DNA
- Analysing AHF's Global Service Delivery
- The Financial Engine of AHF
- Advocacy Priorities and Policy Influence
- Examining Key Controversies and Critiques
- Actionable Insights for G7 and G20 Leaders
The AIDS Healthcare Foundation in Global Health
More than 2.5 million patients. Operations across 49 countries. For G7 and G20 delegates, an HIV organisation at that scale is no longer just part of civil society. It is a transnational delivery actor whose decisions can affect procurement patterns, service continuity, and the balance between public systems and non-state provision.
AHF occupies an unusual position in global health. Many NGOs advocate. Many providers deliver care within a narrow geography. Far fewer combine a large clinical footprint, cross-border operational control, and a confrontational policy voice inside the same institution. That combination places AHF in debates usually reserved for larger global health initiatives and institutional coordination, especially where donors are asking whether funding should prioritise local system capacity, parallel delivery channels, or some mix of both.
The policy relevance of AHF is defined less by its messaging than by what it can operationalise. An organisation with this reach can expand testing and treatment access quickly in some settings, but it can also shape incentives for ministries, donors, and local providers. The key question is whether AHF's scale reduces delivery gaps more effectively than fragmented grant-based models, and in which contexts that scale creates duplication, political friction, or dependence on an external operator.
That is significant for G7 and G20 leaders because HIV governance is increasingly an execution problem, not only a financing problem. Coverage targets, drug access, and retention in care depend on institutions that can keep services running under fiscal pressure and uneven state capacity. AHF therefore deserves assessment as a system actor. The relevant test is not whether it produces visible outputs, but whether its model strengthens national health governance or bypasses it in ways that are harder to sustain.
AHF's strategic weight comes from the interaction between delivery capacity and political agency. Each feature is common on its own. Their combination creates wider implications for international health governance.
Origins and Organisational DNA
From local crisis response to global platform
AHF emerged from the AIDS emergency in Los Angeles in 1987, as noted earlier. That starting point matters for policy analysis because organisations formed under conditions of institutional failure often preserve a crisis-response logic even after they scale internationally. In AHF, that logic appears in a preference for rapid execution, direct control over service channels, and public advocacy that is often sharper than intergovernmental health diplomacy.
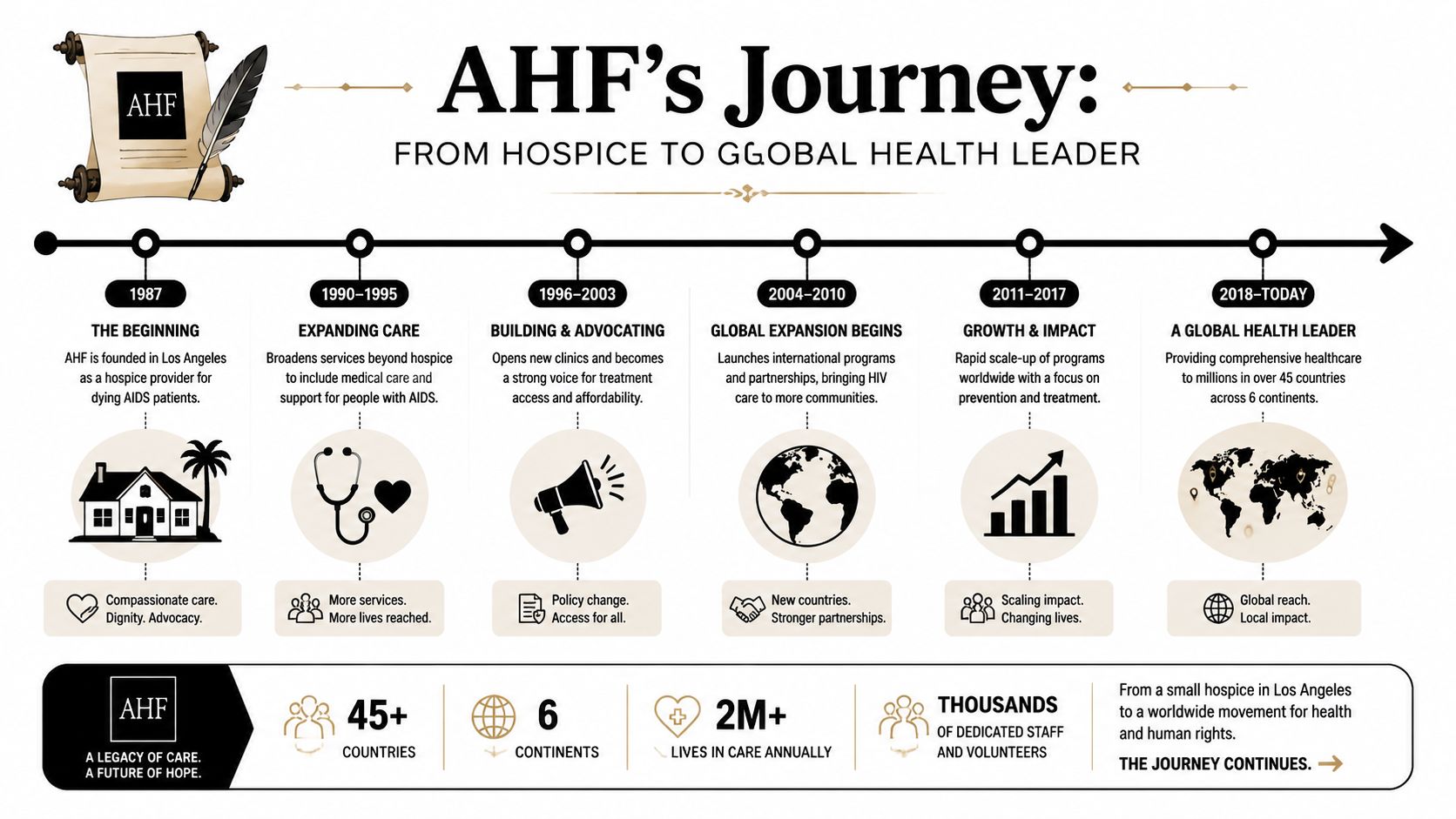
This helps explain why AHF generates both operational praise and political friction. The same institutional traits that can expand access quickly in underserved settings can also create tension with ministries, multilateral agencies, and local providers that prioritise coordination, procurement discipline, and integration with national plans. For G7 and G20 delegates, that is the relevant frame. AHF is not only a service organisation with strong views. It is a case study in how crisis-born health actors evolve into durable governance actors.
That trajectory sits within a broader shift in global health, where non-state organisations increasingly combine financing, implementation, and agenda-setting. The implications of that shift are examined in the evolving role of philanthropy in global health. AHF stands out because it has sustained all three functions at once rather than specialising in only one.
Why the founding logic still matters
Three features appear to define AHF's organisational DNA.
- Integrated HIV service orientation. Available evidence shows AHF focuses on linked functions across the HIV pathway, including testing, prevention, treatment access, and continuity of care, rather than limiting itself to a single intervention.
- Preference for operational control. Its model appears designed to keep multiple parts of delivery within the organisation's influence, which can improve execution speed but can also raise questions about alignment with public systems.
- Advocacy rooted in delivery. AHF's policy positions are shaped by on-the-ground service experience, including practical concerns around testing uptake and treatment access. For readers seeking a patient-level reference point on testing reliability, this guide to HIV test accuracy offers useful context.
These features matter because institutional design shapes policy behaviour. An organisation built to respond quickly to unmet need is likely to value visible action, expansion, and message discipline. Governments have to weigh a wider set of constraints, including fiscal sustainability, interoperability, workforce regulation, and political legitimacy. The result is a recurring governance tension. In some settings, AHF's model can complement state capacity. In others, it can operate alongside public systems in ways that make long-term integration harder.
Policy implication: AHF is best understood as crisis-era service activism scaled into a transnational operating model, with strengths in execution and recurring tensions around system fit.
That interpretation is more useful than treating AHF as either a pure charity or a conventional contractor. For G7 and G20 policymakers, the central question is whether institutions with this organisational DNA should be funded mainly as gap-fillers, integrated more formally into national HIV strategies, or held at greater distance to avoid parallel governance.
Analysing AHF's Global Service Delivery
What the operational footprint signals
Service delivery is where AHF moves from advocacy subject to governance variable. The most relevant independent workforce datapoint comes from Revelio Labs' company profile, which states that AHF describes itself as the largest provider of HIV/AIDS medical care in the world and records 3,877 employees with 2.4% year-on-year growth in workforce size. For policymakers, that matters less as a branding claim than as evidence of institutional depth.
Operational scale changes what an organisation can do. It can standardise workflows, keep programmes running across jurisdictions, and sustain issue attention when donor cycles or political priorities shift. It can also create path dependency. Once a provider reaches a certain size, host systems may begin to depend on it in ways that complicate transition, oversight, or integration.
The strategic question isn't whether AHF reaches patients. It's whether its presence strengthens national HIV architecture or risks creating a parallel one.
A relevant multilateral frame appears in debates on closing gaps in AIDS, tuberculosis and malaria governance. Delivery capacity is essential, but capacity only becomes system value when referral, financing, data, and accountability lines are clear.
Workforce depth and delivery discipline
The staff figure also tells us something about organisational composition. An HIV platform of this sort requires more than clinicians. It depends on administrative coordination, patient navigation, procurement management, pharmacy operations, and communications capacity. That breadth helps explain why AHF can operate as both a service provider and a public advocate.
A short policy reading is useful here:
| Governance lens | Why AHF's scale matters |
|---|---|
| Continuity | A larger workforce supports ongoing service delivery rather than short campaign bursts |
| Negotiating power | Bigger providers can hold firmer positions in funding and policy debates |
| Implementation risk | Large delivery systems can be hard to harmonise with local institutions if roles aren't defined |
Later stages of the HIV care cascade depend heavily on confidence in front-end testing and linkage. For readers looking for a practical explainer on the clinical side of that issue, this guide to HIV test accuracy is a useful companion because it clarifies why testing windows, methods, and interpretation still shape policy effectiveness.
Before considering the video below, one point stands out. AHF's operational significance doesn't come from abstract global presence. It comes from whether it can convert scale into reliable care pathways across varied settings.
Why service design still depends on testing quality
In HIV governance, the first operational failure often appears early in the pathway. People don't enter care because testing access is weak, because trust is low, or because linkage is poorly organised. AHF's broad service model matters because it suggests an effort to control those hand-offs rather than leave them to disconnected institutions.
Operational test: If a provider can't connect prevention, testing, treatment, and linkage in practice, headline footprint tells policymakers less than it seems.
That's why AHF attracts such close scrutiny. It isn't merely offering advocacy on HIV priorities. It is presenting an integrated model that implicitly argues a certain theory of implementation.
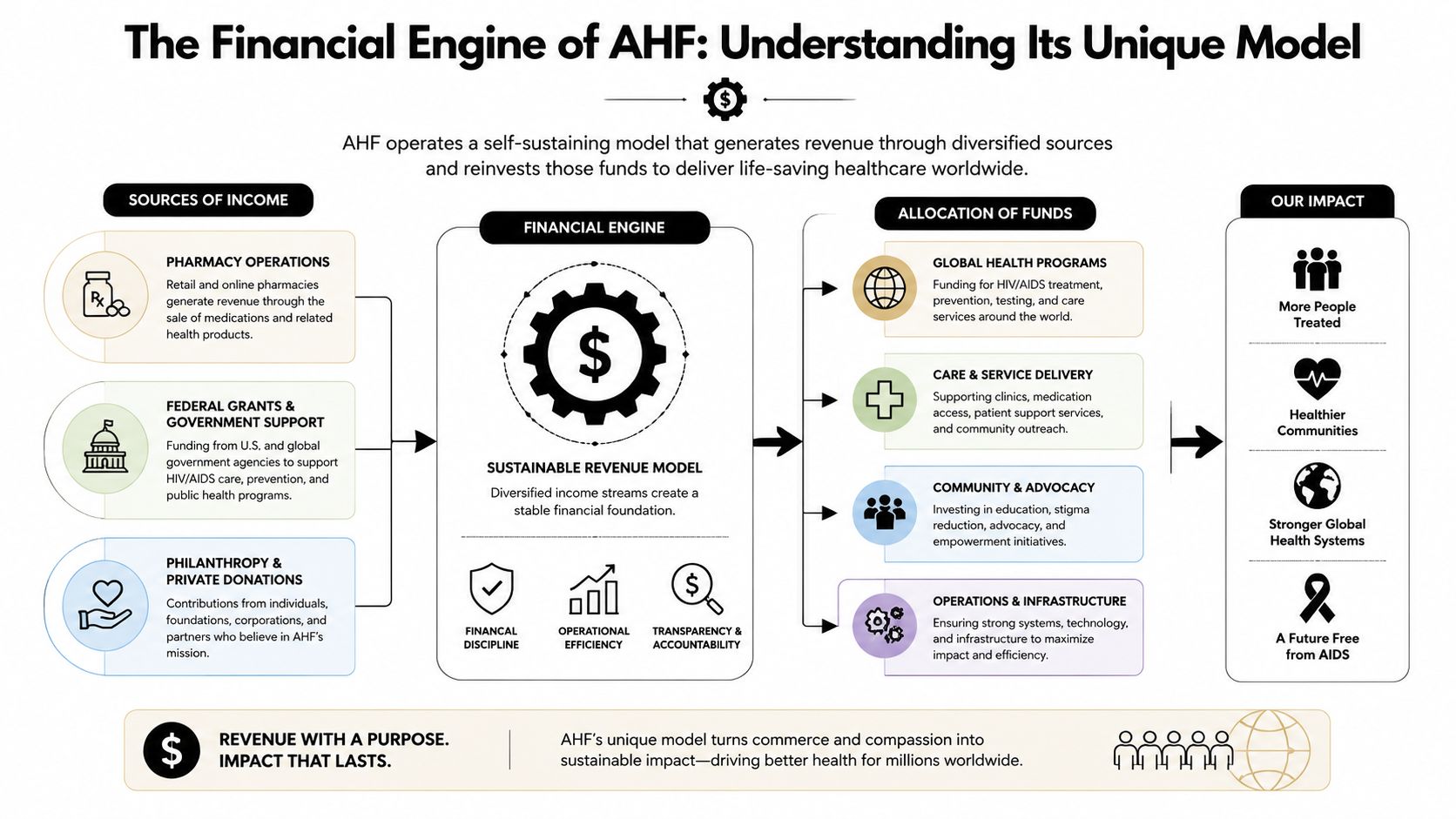
The Financial Engine of AHF
Why policymakers should care about the revenue model
A provider that can finance service delivery and advocacy from a diversified base has more room to shape the terms of policy debate. For G7 and G20 governments, that is the strategic issue with AHF's financial model. It affects not only organisational durability, but also how much influence public funders retain over priorities, reporting standards, and acceptable trade-offs between scale and accountability.
As noted earlier, AHF presents itself as a global nonprofit provider focused on HIV care, testing, prevention, and linkage to treatment. What is less clear from the source set available here is the operating detail that finance ministries and health ministries would normally want before judging transferability. There is no UK-specific breakdown in this material of clinic footprint, patient throughput, procurement terms, or revenue exposure by market. That gap matters because financial strength in one regulatory setting does not automatically translate into policy fit in another.
For the UK and other publicly financed systems, the relevant question is not whether AHF is large. It is whether its financing logic aligns with national commissioning rules, procurement oversight, and statutory public health duties. An organisation built to preserve operating independence may add resilience during donor volatility. The same independence can also complicate alignment if governments expect tighter control over service design, data standards, or target populations.
Governance questions that follow from financial autonomy
A practical assessment starts with incentives.
- Trace alignment. Does the revenue mix support national HIV objectives, or does it encourage concentration in service lines that are easier to sustain financially than they are to justify strategically?
- Examine substitutability. If contracts, reimbursement rules, or access arrangements changed, could the host system absorb those functions without service disruption?
- Test transparency. Do public authorities have sufficient visibility into funding sources, governance controls, and performance expectations to judge value for money?
These questions have wider relevance for multilateral health governance. AHF's model points to a broader tension in global health financing. Organisations that are less dependent on a single donor can preserve continuity when aid priorities shift. They can also press policy positions more aggressively because they are less exposed to donor discipline. For G7 and G20 delegates, that creates a familiar governance problem. Financial resilience can support continuity of care, yet it can also weaken the usual channels through which states steer implementation.
The policy response should be structured oversight rather than reflexive approval or suspicion. For health ministries, grantmakers, and nonprofit operators reviewing their own funding architecture, tools such as Alignmint for nonprofit grant management offer a useful reference point for reporting discipline, audit trails, and clearer lines of accountability in health-focused programmes.
The non-obvious conclusion is that AHF's financing model matters beyond its balance sheet. It is also part of its governance model. Any G7 or G20 assessment of partnership value should therefore test two issues at the same time: whether the model sustains service continuity, and whether it leaves public institutions with enough oversight to protect system-wide goals.
Advocacy Priorities and Policy Influence
Research as a policy instrument
AHF's policy influence is easier to understand when its research function is treated as part of its operating strategy rather than as a separate academic adjunct. On its research page, AHF frames its work around behavioural, biomedical, and social-science methods for HIV and STI prevention, testing, treatment, and linkage to care. For UK and wider G7 audiences, that is the technically relevant detail because it mirrors the evidence-led architecture through which HIV policy is usually justified.
That matters for international governance because methodology shapes legitimacy. Organisations that can point to behavioural, biomedical, and social-science approaches are better placed to argue that they are addressing the full care cascade rather than only one intervention point. In summit settings, that broadens influence. AHF can contribute to debates on prevention messaging, testing models, treatment access, and system design using a common evidence vocabulary familiar to governments and multilateral agencies.
Still, a research frame doesn't settle policy disputes. It structures them.
Where influence can align or clash with governments
AHF's advocacy style tends to matter most in three kinds of policy environment:
- Access debates where medicines, prevention tools, or treatment pathways become politically contested.
- Funding debates where governments want cost control and civil society actors want urgency and expansion.
- Governance debates where the issue isn't whether HIV services matter, but who should deliver them and under what accountability rules.
This is why the organisation can appear both indispensable and difficult. A provider with operating experience often sees implementation barriers earlier than distant funders do. But the same provider may press its case in ways that public authorities see as disruptive, especially when negotiations require coalition discipline.
Research gives AHF a language of technical authority. Delivery gives it standing. Advocacy gives it reach. The interaction of all three is where influence accumulates.
For G7 and G20 delegates, the key insight is that AHF's interventions shouldn't be read as generic NGO positioning. They are better understood as attempts to shape policy environments around a specific theory of HIV delivery, one grounded in integrated services and strong institutional visibility.
Examining Key Controversies and Critiques
The core policy tensions
For G7 and G20 policymakers, the relevant question is not whether AHF is unusually visible. It is whether a large, vertically integrated HIV organisation strengthens national delivery systems or complicates them. That distinction matters because global health governance now depends less on formal mandates alone and more on how major non-state actors fit into public financing, regulation, and accountability.
The primary tension involves integration versus parallelism. Large nonprofit providers can close access gaps quickly, especially where public systems are under strain or politically neglected. The risk is institutional fragmentation. If referral rules, data sharing, procurement decisions, or commissioning arrangements are weak, a high-capacity NGO can begin to operate beside the public system rather than within it. For donors and ministries, that can improve short-term coverage while reducing long-term system coherence.
A second tension concerns pressure politics versus coalition management. AHF's advocacy style has often been designed to force contested issues into public view. That approach can shift policy agendas, particularly when governments delay action or protect incumbent interests. It can also impose costs. Ministries, municipal health authorities, and civil society coalitions often need negotiated settlements, not only public pressure. An actor that is effective at agenda disruption may be harder to absorb into coordinated implementation.
The third tension is autonomy versus transparency. Organisations with strong internal capacity can act faster than many public bureaucracies. Speed, however, does not remove the need for scrutiny. Governments still need visibility into incentives, service substitution effects, and operational trade-offs, especially when one organisation combines advocacy, service delivery, and institutional brand power.
These tensions are not unique to AHF. They are part of a wider governance problem in global health. As large NGOs take on functions once associated mainly with states or multilateral implementers, the policy debate shifts from charitable intent to system effects.
The UK lens remains evidence-constrained
The source base supports a general characterisation of AHF as a large global HIV provider and advocate, as noted earlier. It does not provide UK-specific operating data on clinic footprint, patient volume, commissioning arrangements, or procurement performance. That limits what analysts can responsibly claim about Britain. It also improves the quality of the policy assessment, because it forces attention onto institutional fit rather than organisational reputation.
In the UK, the central issue would be compatibility with existing governance architecture. Any AHF-facing role would need to align with NHS treatment pathways, local authority public health commissioning, sexual health service provision, and the established position of domestic charities. A globally scaled model does not automatically translate into added value inside a system with dense public oversight and mature provider networks.
That makes three questions especially important:
- Which populations are underserved, based on demonstrated gaps in access, retention, or prevention uptake?
- Which local systems would absorb or resist an additional actor, given variation across cities, commissioners, and provider markets?
- Which function would AHF perform better than existing arrangements, whether outreach, testing, treatment linkage, procurement pressure, or policy advocacy?
For G7 and G20 delegates, the wider implication is clear. Controversy around AHF should not be read only as a dispute about organisational style. It is also a test case in how governments evaluate high-capacity NGOs that operate across advocacy and delivery at once. Where the rules are clear, data sharing is enforceable, and public objectives are explicit, such actors can add pressure and capacity. Where those conditions are weak, the same model can intensify fragmentation and political conflict.
The absence of UK-specific operating data does not weaken the analysis. It narrows the claims to the ones policymakers can defend, and directs attention to governance design rather than institutional mythology.
Actionable Insights for G7 and G20 Leaders
Treat AHF as a system actor, not a single stakeholder
AHF's rise points to a broader trend in global health governance. Some NGOs now combine enough scale, staffing, and service integration to function as quasi-system actors. They influence not just advocacy debates, but also delivery norms, workforce patterns, and the politics of access. G7 and G20 governments should update their engagement models accordingly.
That starts with classification. When ministries engage AHF, they shouldn't place it in a generic civil society bucket. It should be assessed across at least three dimensions at once: provider capacity, advocacy influence, and compatibility with national governance structures.
A practical approach looks like this:
| Policy task | Recommended question |
|---|---|
| Partnership design | Does AHF fill a delivery gap that the public system cannot close quickly on its own? |
| Political management | Are there structured channels to handle disagreements before they become public stand-offs? |
| Accountability | Are data sharing, referral, and oversight arrangements explicit enough to protect system coherence? |
Use country fit as the central test
The most overlooked lesson is that scale doesn't equal transferability. A model that works across many jurisdictions can still fit poorly within a specific national architecture. That's especially relevant in the UK. The source set notes a frequently missed angle: how well AHF-style HIV services reach underserved groups in Britain, especially Black African communities, gay and bisexual men, and people outside London, while also noting that new diagnoses remain concentrated in London and among key risk groups according to the framing summarised in the available UK-facing reference context.
For G7 and G20 leaders, that yields five concrete takeaways:
- Don't reward scale alone. Reward measurable fit with national pathways.
- Interrogate duplication risk. Large nonprofits can help close gaps, but only if roles are clearly differentiated.
- Value integrated service models. Prevention, testing, treatment, and linkage work best when hand-offs are intentional.
- Expect political assertiveness. Institutions built through crisis response rarely confine themselves to quiet implementation.
- Keep underserved populations central. National averages can obscure where delivery models succeed or fail.
The larger conclusion is that AHF should neither be romanticised nor dismissed. It represents a durable form of health power that multilateral institutions will confront more often in the coming decade. The right response is governed partnership: clear terms, evidence-based scrutiny, and a willingness to use capable delivery actors without surrendering public accountability.
For more policy analysis on global health governance, summit priorities, and multilateral decision-making, visit Global Governance Media.