

By Daniel Hart, Senior Policy Analyst
The most consequential health partners in Africa aren’t always the ones that dominate donor branding in G7 capitals. They’re often the institutions that can convert local trust, workforce development, disease surveillance, and last-mile delivery into system-wide resilience. On the available evidence, amref health africa belongs in that category.
That conclusion isn’t rhetorical. In 2024, Amref Health Africa implemented 172 projects across 37 African countries, reached 19.1 million people directly, trained or equipped 153,010 healthcare workers, and delivered over 24.9 million service contacts, according to Amref Health Africa’s 2024 annual report abridged version. For G20 delegates, that scale matters because it sits at the intersection of pandemic preparedness, primary healthcare, labour force development, and humanitarian response.
The counterintuitive point is this. If governments treat Amref only as an implementing NGO, they’ll undervalue it. The stronger reading is that it operates as health infrastructure in organisational form. Its programmes don’t just deliver services. They also train workers, generate field intelligence, and create operational channels that multilateral actors can use when formal systems are under pressure.
Table of Contents
- An Indispensable Partner in Global Health Security
- Understanding Amref's Organisational DNA
- Programmatic Pillars and Continental Footprint
- Measuring Success A Data-Driven Impact Analysis
- Shaping Policy from the Grassroots to Global Summits
- Navigating Risks Criticisms and Accountability
- Strategic Pathways for Engagement and Investment
An Indispensable Partner in Global Health Security
Global health security is often discussed through summit communiqués, emergency financing vehicles, and cross-border surveillance frameworks. Yet those instruments only work when capable delivery partners can translate them into functioning care pathways. That’s where amref health africa matters.
Its importance lies in the combination of continental reach, workforce training, and community-level implementation capacity. For multilateral actors, those capabilities form the missing middle between high-level financing and frontline delivery. A health system can’t absorb external support if it lacks trusted local channels, trained workers, and actionable local data.
This is also why Amref’s relevance extends beyond Africa policy. It touches broader G20 concerns about economic resilience, supply shocks, migration pressures linked to health insecurity, and the global spread of infectious threats. A partner that strengthens primary healthcare and disease response capacity in multiple countries contributes to international stability, not only local service provision.
Practical rule: When a health partner can train workers, deliver services, and inform surveillance at scale, governments should assess it as part of the security architecture, not just the aid ecosystem.
That framing aligns with a wider argument in this analysis of the global health security cosmopolitan moment. Health security now depends on institutions that can connect local legitimacy with international coordination. Amref’s profile fits that requirement unusually well.
For G20 delegates, the strategic implication is straightforward. Engagement with amref health africa shouldn’t be limited to project-by-project funding decisions. It should be considered within broader discussions on workforce resilience, anticipatory action, and the practical delivery mechanisms needed to make multilateral health commitments credible.
Understanding Amref's Organisational DNA
Amref’s strategic weight comes from institutional design, not only programme volume. For G20 policymakers assessing delivery partners, the central question is whether an organisation can convert external financing into trusted implementation across political, geographic, and administrative boundaries. Amref’s structure suggests that it often can.

Why its Africa-led identity matters
Amref is widely described as the largest Africa-led international health NGO. That status matters for more than institutional branding. It shapes who sets priorities, how implementation risks are judged, and whether programmes are designed with realistic assumptions about state capacity, local politics, and community trust.
That matters in multilateral cooperation because many health partnerships fail at the point where technical design meets administrative reality. An organisation with leadership, operating history, and political fluency rooted in the region is often better placed to judge what a ministry can absorb, what a district can supervise, and what a community will accept. In practice, that can affect procurement timing, referral uptake, workforce retention, and the credibility of public messaging during outbreaks.
Three implications follow for external funders and official agencies.
- Legitimacy travels further than access. An Africa-led institution can enter policy conversations without carrying the same political baggage as externally directed implementers. That can improve cooperation across ministries and subnational authorities.
- Judgement improves implementation. Contextual knowledge does not guarantee success, but it can reduce design errors that commonly weaken donor-funded programmes.
- Partnerships become more durable. Organisations seen as regionally grounded are often better positioned to sustain working relationships through electoral change, fiscal stress, or shifts in donor priorities.
This should not be romanticised. Regional leadership does not remove fiduciary risk, governance problems, or uneven performance across countries. It does, however, change the probability that programme design will match operational conditions. For health security investors, that is a material advantage.
What policymakers should infer from the funding picture
The public material available to outside analysts does not provide a full, disaggregated picture of UK-specific funding flows, bilateral grant exposure, or formal alignment with FCDO priorities. That gap matters. It limits the ability of policymakers to assess concentration risk, co-financing opportunities, and the extent to which Amref is positioned inside broader donor coordination frameworks.
The more useful reading is institutional rather than transactional. Amref appears to combine three features that multilateral actors usually seek separately: regional legitimacy, delivery capacity, and a programme model tied to workforce and system strengthening. Its 2022 annual report reinforces that picture by showing continuity in organisational focus, including health workforce development and data-related functions, rather than a narrow reliance on one disease vertical or a short-lived emergency role.
| Layer | What it suggests | Why it matters |
|---|---|---|
| Institutional identity | Africa-led and regionally embedded | Improves contextual judgement and political acceptability |
| Programme model | Links service delivery with workforce and system support | Increases the odds that funding produces effects beyond single projects |
| Partnership visibility | External relationships exist, but some bilateral details remain unclear in public documentation | Points to a transparency agenda for governments planning long-term engagement |
A mature partner is not defined only by expenditure levels. It is defined by whether it can preserve operational coherence when donor preferences shift, crises overlap, or governments ask it to align with national plans rather than stand-alone projects.
For G20 delegates, the strategic conclusion is clear. Amref should be assessed as part of the implementation architecture that sits between global commitments and local execution. That makes questions of governance, transparency, and institutional resilience just as important as headline programme reach.
Programmatic Pillars and Continental Footprint
Amref’s continental relevance rests on a practical fact. It operates across multiple layers of the health system at once, giving governments and donors a partner that can deliver services, reinforce frontline capacity, and improve operational visibility in the same geography.

Service delivery with system effects
The programme mix described in Amref’s public reporting spans primary care access, infectious disease response, child immunisation, tuberculosis screening, malaria treatment, and support for people living with HIV. For a policy audience, the strategic value lies in how these functions interact. Programmes built through shared community networks, referral channels, and training systems can produce wider system benefits than stand-alone projects designed around a single disease target.
This matters for G7 and G20 partners that are trying to reconcile vertical financing with broader health security goals. A delivery platform that can support outbreak response, routine services, and population-level prevention through overlapping field infrastructure reduces fragmentation at country level. It also gives finance and health ministries a clearer implementation counterpart when external funding streams multiply.
Community health workers sit at the center of that model. In many settings, they are the operational link between national health plans and households that face distance, cost, or information barriers to facility-based care. For governments, that means earlier case identification, more reliable follow-up, and better referral continuity. For donors, it means that investments in one programme area can strengthen surveillance and service uptake in another.
A more policy-relevant way to read Amref’s footprint is through three connected functions:
- Frontline reach: Extending prevention, screening, referral, and basic services into underserved communities.
- Workforce standardisation: Using training and protocol support to improve consistency across dispersed delivery sites.
- Operational feedback: Converting field activity into information that can guide targeting, supervision, and resource allocation.
That combination helps explain why Amref appears repeatedly in country contexts where health systems face overlapping burdens rather than a single emergency.
Technology as operational infrastructure
The organisation’s more persuasive innovation story is not digital branding. It is whether technology changes decisions in the field.
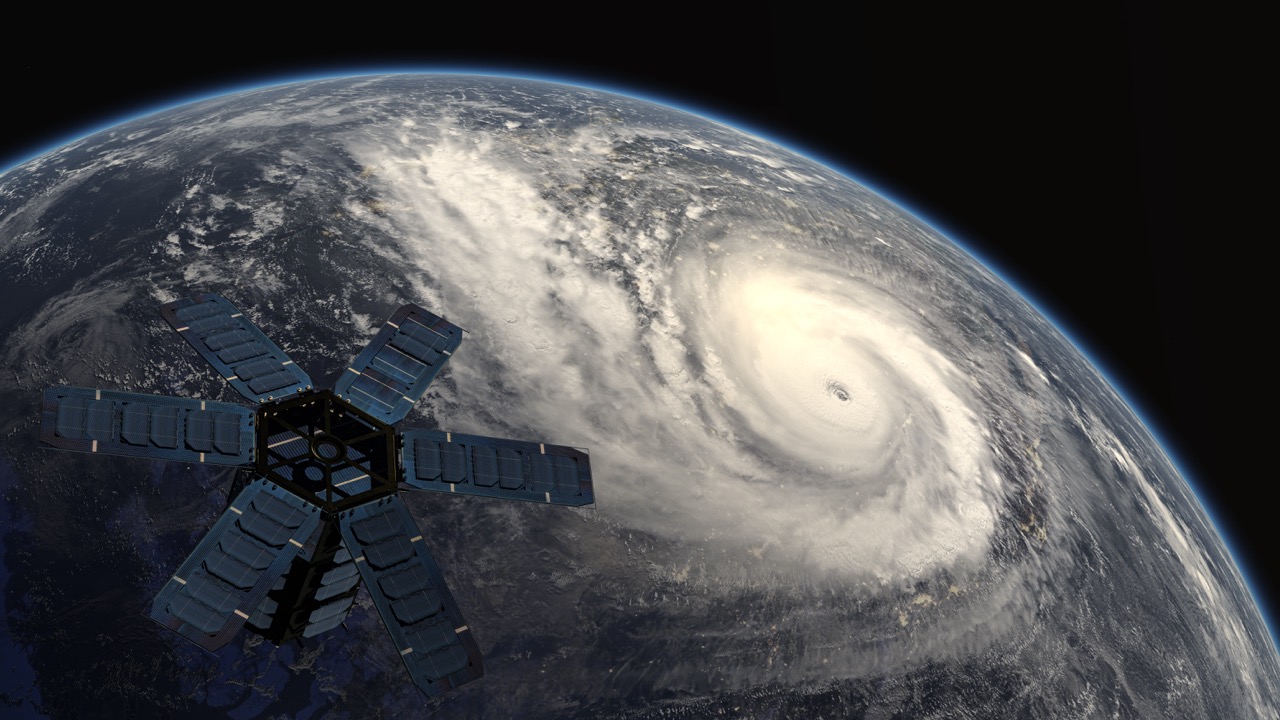
One example is its advanced machine learning model using Microsoft Azure, which integrates clinical health data with satellite imagery to predict malnutrition hotspots across Kenya and enable pre-positioning of aid, as described in Microsoft’s case study on Amref’s predictive analytics work. The policy implication is straightforward. Better anticipation can improve the timing of response and reduce the cost of acting only after nutritional stress becomes visible in facilities or mortality data.
A second example is the Leap mLearning platform, which has been used to support training, protocol uptake, and data capture among community health workers. Public reporting has also linked that digitally supported approach to tuberculosis work, including Amref’s support for more than 3,000 community health volunteers across 14 counties in Kenya to screen over 1 million people for TB over a three-year period. Those details are reported in the Elsevier Foundation profile on Amref’s data-driven community health work. The broader significance is less about the platform itself than about what it signals. Amref is trying to make community health more legible to managers and funders, which is a recurring weakness in primary health care financing.
The video below offers additional context on the organisation’s field-facing work and public identity.
For multilateral partners, the central takeaway is strategic. Amref should be assessed not only as a service implementer, but as part of the execution layer between global financing commitments and local health system performance. That position matters in current debates over pandemic preparedness, community health financing, and how to fund institutions that can convert fragmented external support into usable delivery capacity.
Measuring Success A Data-Driven Impact Analysis
For G20 and G7 policymakers, the strategic test is straightforward. Can Amref convert donor capital, political commitments, and local delivery capacity into measurable health results at scale? Its latest reported figures suggest that it can, and that matters for current debates on health security financing, primary care delivery, and African institutional execution.
What the 2024 figures show
According to Amref Health Africa’s 2024 annual report abridged version, the organisation implemented 172 projects across 37 African countries, reached 19.1 million people directly, indirectly affected 39.4 million people, trained or equipped 153,010 healthcare workers, and delivered more than 24.9 million service contacts.
Those numbers are large, but their policy value depends on composition rather than volume alone.
| Indicator | Reported result | Strategic reading |
|---|---|---|
| Projects implemented | 172 | Operational breadth across multiple health systems |
| Countries covered | 37 | Experience across varied political and epidemiological settings |
| Direct reach | 19.1 million | Significant programme-level exposure |
| Indirect impact | 39.4 million | Effects extending beyond immediate service users |
| Healthcare workers trained or equipped | 153,010 | Investment in delivery capacity, not only campaign output |
| Service contacts | Over 24.9 million | Repeated interaction with communities and health systems |
The same report indicates that 61% of services, or 15.2 million, focused on health access and coverage, while 36%, or 9.1 million, were tied to climate change and health strategic objectives. That split is analytically important. It suggests Amref is positioning itself at the intersection of routine service provision and resilience planning, a combination that aligns with the financing logic behind a new deal for African health security.
Outcome metrics matter more than aggregate reach because they show whether contact is translated into clinical continuity and public health effect.
On HIV, the same report states that Amref’s interventions initiated 98,881 people living with HIV on antiretroviral therapy in Kenya and Tanzania, with a 95% treatment linkage rate and 98% viral load suppression. Those are not outreach metrics. They point to performance in the harder part of programme delivery, keeping patients connected to treatment long enough to produce measurable outcomes.
Other reported results reinforce that pattern. Amref supported 388,764 child immunisations in Kenya, Uganda, and West Africa, screened 619,000 people for tuberculosis in Kenya and Tanzania, facilitated more than 25 million COVID-19 vaccine doses, and treated 779,000 confirmed malaria cases across Kenya, Malawi, South Sudan, Uganda, and Zambia through community outreach and community health worker-led efforts.
For sovereign donors and multilateral funds, the wider implication is clear. Amref appears strongest where global health financing often struggles most: translating earmarked support into workforce deployment, follow-up, and repeat service contact across dispersed settings. That makes it more than a grant recipient. It makes it a plausible implementation partner for longer-horizon investments in preparedness, primary care, and delivery system resilience.
Shaping Policy from the Grassroots to Global Summits
The most insightful reading of amref health africa is that it occupies two spaces at once. It is a delivery organisation, but it is also a policy translator. It takes field experience from communities and health systems, then converts that experience into positions that matter in regional and global forums.

Operational legitimacy becomes policy influence
That translation role matters because many global health debates are distorted by distance. Financing conversations in high-income capitals often separate preparedness from primary care, and innovation from workforce constraints. Organisations like Amref can challenge that split because they work where those issues collide in practice.
Its field presence gives it credibility on several policy questions that recur in G20 processes:
- Universal health coverage: Community systems and frontline labour supply determine whether formal coverage commitments become real access.
- Pandemic preparedness: Early warning, local trust, and deployable workers matter before emergency financing can have effect.
- Health financing: Donors often underinvest in the operating systems that make targeted interventions work.
- Climate and health: Service delivery increasingly has to account for climate-linked shocks and population vulnerability.
This is why service delivery experience can produce policy relevance. The organisation can speak to what ministries, districts, and community networks can absorb. That’s often more useful than abstract consensus language produced far from implementation settings.
Why G20 processes should pay attention
For summit diplomacy, the mistake would be to confine Amref to side-event visibility while excluding it from upstream agenda design. A partner with deep field intelligence can help governments ask better questions before they commit money.
That’s especially true for health security discussions that seek a stronger African voice in agenda setting. The broader policy case for this approach is well captured in the argument for a new deal for African health security. The central issue isn’t representation alone. It’s whether policy is being shaped by actors who understand the mechanics of delivery.
A useful test for policymakers is simple. When an institution can show where referral chains break, where community trust is thin, where data arrives late, and where workforce shortages become programme failure, it has earned a seat in strategy formation. Amref appears to meet that test.
Global health policy improves when organisations that carry implementation risk help shape financing and governance rules.
That doesn’t mean governments should outsource strategy to NGOs. It means they should build policy processes that incorporate operational evidence earlier and more seriously.
Navigating Risks Criticisms and Accountability
For G20 policymakers, the hardest question is not whether Amref adds value. It is whether the current financing and oversight model is capable of sustaining the kind of Africa-based institution that health security strategies say they need.
Funding pressure is a systemic problem, not an isolated organisational issue
As of March 2026, Amref said it had “weathered financial cuts with unwavering persistence” in its article on new realities in a funding-starved health sector. Read narrowly, that is a statement about organisational resilience. Read strategically, it is a warning about the design flaws of global health finance.
The contradiction is familiar across the multilateral system. Governments and donors call for locally rooted delivery partners, stronger primary care, and better preparedness. Yet many funding streams remain short-term, earmarked, and vulnerable to political shifts in capitals far from implementation. That structure rewards visible outputs over institutional continuity.
For an organisation like Amref, the policy consequences are concrete. Staff retention becomes harder. Training pipelines are interrupted. Community trust can erode when services expand and contract with donor cycles. Preparedness also weakens because institutions under financial strain protect current programmes before they invest in surge capacity, data systems, or local stock readiness.
This matters well beyond one NGO. It goes to the unresolved financing debate around who pays for continuity in public health systems, a question closely tied to broader discussions on financing universal health coverage and health system resilience.
Accountability runs to donors, governments, and communities at the same time
Accountability is often framed too narrowly in aid discussions. Upward reporting to donors matters, especially where public money and pooled funds are involved. But for delivery partners working through district systems and community networks, legitimacy also depends on whether local actors regard the organisation as responsive, predictable, and aligned with public priorities.
Those obligations do not always point in the same direction.
Donors often prefer metrics that are standardised, rapid, and easy to compare across countries. Health ministries and frontline systems often need something different: continuity, flexibility, and adaptation to uneven local conditions. Community actors may place the highest value on trust, cultural fit, and whether promised services materialise over time. Strong performance therefore depends not only on reporting discipline, but on the ability to balance competing accountabilities without reducing programmes to what is easiest to count.
A sharper assessment of Amref should therefore focus on a specific set of risks:
| Issue | Why it matters |
|---|---|
| Funding volatility | Interrupts workforce planning, training continuity, and community-facing services |
| Operating complexity | Work in remote, fragile, or politically sensitive settings raises delivery and compliance risk |
| Public transparency limits | Some partnership and financing details are not always easy to track externally |
| Accountability overload | Multiple reporting demands can pull attention away from implementation quality |
None of these concerns is unique to Amref, and that is precisely why they deserve policy attention. They reflect structural pressures facing many Africa-based health partners that sit between community delivery, national systems, and donor compliance regimes.
The strategic implication is straightforward. If G7 and G20 governments want credible regional institutions to carry more implementation responsibility, they will need funding arrangements and accountability frameworks that match operational reality. Otherwise, the multilateral system will continue to demand local ownership while financing short-term performance theatre.
Strategic Pathways for Engagement and Investment
For G20 governments, the strategic question is allocation, not recognition. Amref Health Africa already occupies a position that many donors say they want to support: an Africa-based institution with delivery capacity, policy access, and operational experience across the gap between community health systems and national reform agendas. The test for external partners is whether their financing models reinforce those strengths or weaken them through short cycles, fragmented mandates, and reporting burdens that privilege donor control over implementation quality.
A stronger engagement model starts with time horizon. Health workforce development, community referral systems, and locally embedded disease surveillance do not produce stable results on annual political calendars. They require predictable financing, space for adaptation, and procurement rules that fit difficult operating environments. For multilateral lenders and bilateral agencies, this points to a simple conclusion. If the objective is resilience rather than episodic output, partnership design matters as much as budget size.
Four routes stand out.
First, co-invest in workforce systems rather than treating frontline staff as a delivery input to be activated only during emergencies. Amref’s long-standing focus on training, supervision, and professional development makes it a credible vehicle for strengthening the labour base of primary care. That aligns directly with G20 concerns about pandemic preparedness, routine service continuity, and the medium-term shortage of skilled health workers across many low- and middle-income settings.
Second, use Amref more deliberately in anticipatory action. Where institutions can convert local monitoring into earlier intervention, donors should fund the full chain from community data collection to operational response. Waiting for formal crisis designation often costs more and reaches populations later.
Third, shift from short grant cycles to multi-year frameworks tied to system outcomes. This does not mean weaker accountability. It means judging performance against whether training systems hold, referral pathways improve, and local delivery capacity expands over time. Those are harder tests than counting short-term activities, but they are more relevant to state capability and health security.
Fourth, bring implementation partners into financing design earlier. Institutions with direct knowledge of workforce bottlenecks, absorption constraints, and local political conditions should shape programme architecture before targets are fixed. Early input reduces the common pattern in which centrally designed initiatives arrive with unrealistic delivery assumptions and then compensate with heavier compliance demands.
For policymakers, the practical implications are clear:
- Back workforce continuity: finance training, supervision, and retention functions, not only campaign delivery.
- Fund integrated primary care platforms: avoid separating infectious disease work from maternal health, community outreach, and routine services when delivery systems are shared.
- Support operational intelligence: invest in local data systems that inform decisions fast enough to prevent deterioration.
- Create structured policy feedback: include experienced implementers in agenda setting, financing design, and mid-course correction.
Public visibility into bilateral partnership models also remains uneven. As noted earlier, available material does not always make it easy to trace how specific government funding relationships map onto stated policy goals. That matters for more than transparency. It affects allocation quality, because governments cannot assess whether their aid architecture is backing institutions capable of absorbing funds, adapting programmes, and sustaining delivery in difficult settings.
This is why wider debates on financing universal health coverage are directly relevant to Amref. The central issue is not only mobilising more money. It is choosing channels that connect financing to implementation capacity, local legitimacy, and policy learning.
The policy conclusion is straightforward. G7 and G20 actors should treat Amref Health Africa as a partner for system resilience and regional health security, then match that recognition with longer funding horizons, earlier institutional consultation, and clearer disclosure around bilateral support. That would improve donor effectiveness and strengthen the multilateral health architecture that increasingly depends on capable regional implementers.