


The 2025 global health audit conducted by the Lancet captures the complex dynamics of the international health landscape and the macro-level burden of disease. It shows a decrease in the burden of communicable diseases juxtaposed against an increase in the burden of non-communicable diseases. It also shows an overall improvement in mortality rates, contrasted with a decline in the quality of life. Against a backdrop of health and development aid underfunding, geopolitical and climate instability, and digital misinformation and disinformation, calls for prioritising the systemic and social determinants of health are more pertinent than ever. The G7, as a longstanding member of the global governance health network, plays a key role in defending and strengthening global health systems.
Deliberation
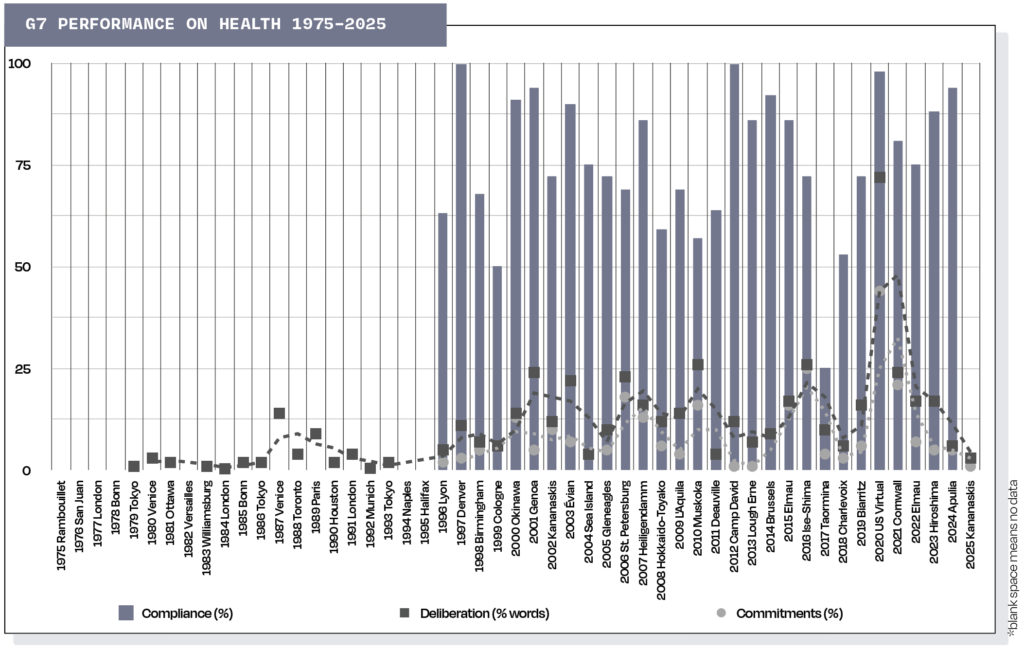
For nearly five decades, G7 leaders have participated in global health governance. Starting in 1979 through to the mid-1990s, they primarily publicly deliberated on the HIV/AIDS epidemic, on infectious diseases such as polio, malaria and tuberculosis, and on ageing and health research. These health issues took an average of 3% of the G7’s communiqués.
The world has changed significantly since then. Reflecting this, from 1996 to 2015 G7 attention to health jumped, averaging 13% per summit. The early years of this period ushered in a strong link to development, with Africa becoming a focal point, alongside nutritional health and women’s health.
The most recent decade, from 2016 to 2025, saw a rising trend, with an average of 18%. The Ebola, Zika and Covid-19 viruses characterised this era, bringing communicable diseases back to the fore. This encouraged a move towards strengthening health systems for better preparedness and response to global health crises, including climate change impacts and mental health.
Commitments
Despite its longstanding deliberations on health, the G7’s first actionable commitment did not come until 1996. Since then, G7 leaders have made 612 health commitments. Only energy and development account for more. There has been a small rising trend in the number of health commitments made over time. From 1996 to 2015, health commitments averaged 7% per summit. From 2016 to 2025, they averaged 12%. The peak came in 2020, when the vast majority of the communiqué reflected the Covid-19 crisis, with 44% of the commitments.
Compliance
Conversely, compliance with the 106 health commitments assessed by the G7 Research Group averages 76%, but has slightly declined over time. From 1996 to 2015, it averaged 77%. From 2016 to 2024, it declined to 73%. By December 2025, compliance for the health-related commitment made at 2025 Kananaskis Summit averaged 69%.
By member, Canada leads the G7’s health compliance with 88%. The United Kingdom follows closely with 87%. The United States and European Union come next with 86% each. In the mid-range are Germany with 77%, followed by Japan and France with 75% each. At the bottom are Italy with 63% and Russia with 56% (when it was a G7 member from 1998 to 2013).
Recommendations
From these findings, several observations can be made. First, G7 health commitments fall into three broad categories. Communicable diseases, including HIV/AIDS, Ebola and Covid-19, average 78% compliance. Non-communicable diseases related to ageing, reproductive health and mental health average 75%. In between, health systems, universal health coverage, capacity building, and access and affordability average 77%.
Second, breaking these categories down further reveals G7 preferences for resource allocation. For communicable diseases, the acute crisis of Covid-19 captured the G7’s resources, resulting in high 90% compliance. The infectious diseases of HIV/AIDS, malaria, tuberculosis and polio combined have been on the G7’s agenda the longest, averaging 79% compliance.
On non-communicable diseases, active ageing risk factors average 79%. This is followed by women’s health with 74% and mental health with 65%. Compliance with the 2025 commitment on capacity building to address wildfire exposure averaged 69% by December 2025.
On health systems strengthening generally, compliance averages 100%. However, strengthening climate-resilient health systems has lower compliance of 70%. Access and affordability issues average
85%, and capacity building and healthcare worker training together average 69%.
Standing out are the compliance gaps on mental health, capacity building, healthcare worker supports, climate-resilient health systems and women’s health. These findings align with the Lancet’s research showing increasing non-communicable diseases globally, alongside rising climate change disasters and health risks, and the historical neglect of women’s health. G7 leaders at Évian should therefore increase their support for non-communicable disease issues. This support should target climate, gender, mental health and vulnerable populations.
