

By Dr Alex Mercer
The most important shift in diagnostics over the past few years wasn't a breakthrough machine in a hospital basement. It was the normalisation of diagnosis happening away from the clinic, yet still inside a governed health system. In the UK, the NHS Test and Trace pathway processed 381,409 positive results by the end of July 2020, demonstrating that remote diagnostic infrastructure could operate at national scale for public health control, not merely for convenience (ScienceDirect analysis of the UK model).
That matters for G7 and G20 leaders because remote diagnostic technologies now sit at the intersection of health security, system resilience, workforce pressure, and economic continuity. They are no longer just telehealth accessories. They are operating systems for earlier detection, distributed care, and faster state response. The strategic question is no longer whether countries should use them. It is how governments should regulate, finance, and align them across borders without deepening inequity or losing clinical control.
Table of Contents
- The New Frontier of Global Health Security
- The Four Pillars of Remote Diagnostics
- Global Use Cases and Strategic Impact
- The Governance Challenge of Cross-Border Hurdles
- Bridging the Gaps in Equity Workforce and Finance
- Case Study The UKs Integrated Diagnostics Model
- A G7/G20 Roadmap for Secure and Equitable Adoption
The New Frontier of Global Health Security
Diagnostic capacity has usually been discussed as a technical input. That framing is now too narrow. The OECD's Health at a Glance 2025 highlights significant cross-country variation in diagnostic infrastructure, underscoring that diagnostic capacity is a system-level determinant of timely treatment and service performance (OECD diagnostic technologies chapter).
For ministers, the strategic implication is clear. A country that can move diagnosis closer to the patient without losing quality gains more than convenience. It gains surge capacity, earlier intervention, and greater resilience when hospitals are under pressure.
Health security now depends on distributed diagnosis
Remote diagnostics make health systems less dependent on a single point of care. Instead of waiting for episodic contact inside hospitals or clinics, governments can build pathways where testing, monitoring, triage, and escalation happen across homes, pharmacies, ambulances, and virtual platforms.
That changes the state's operating posture in three ways:
- Preparedness improves: Authorities can route data from distributed settings into national oversight structures faster.
- Access broadens: Patients who face travel, waiting-time, or workforce barriers can enter the system earlier.
- System pressure shifts: Acute services can reserve in-person capacity for cases where in-person care is essential.
Remote diagnostics should be treated as critical public infrastructure, not as an optional digital service layer.
The political choice is about governance, not gadgets
The temptation is to frame the sector as a contest of devices, apps, and algorithms. That's the wrong level of analysis. The harder question is whether governments can build rules that support safety, interoperability, and equitable payment while allowing innovation to scale.
For G7 and G20 countries, this is especially urgent because these states shape the regulatory norms, procurement standards, and financing expectations that many others later follow. If they align around a workable model, remote diagnostics can become a stabilising force in global health systems. If they don't, countries will inherit a fragmented market of incompatible tools, uneven evidence standards, and widening digital exclusion.
The Four Pillars of Remote Diagnostics
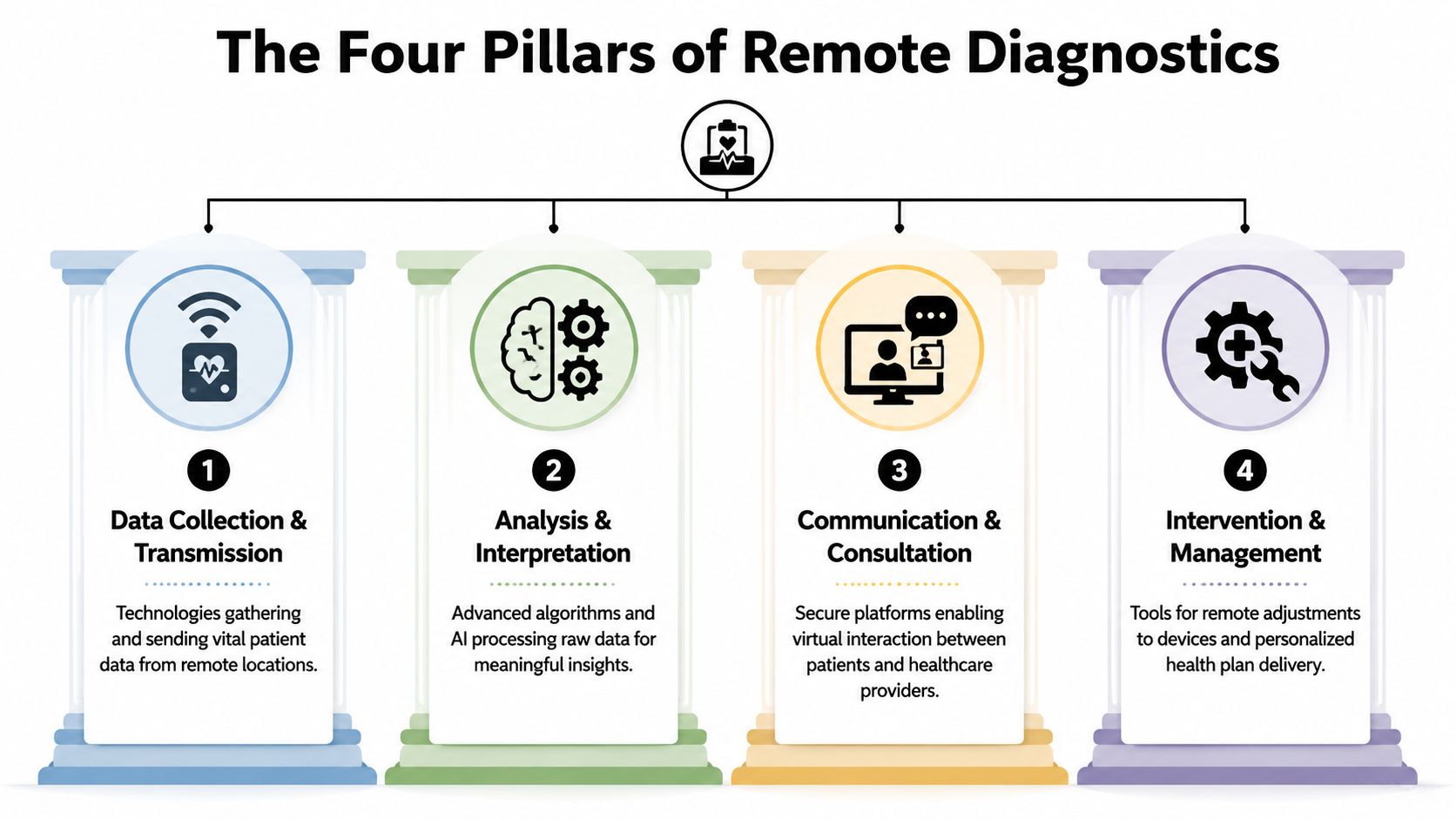
Remote diagnostics are easiest to govern when they're understood as a functional ecosystem rather than a loose collection of products. A useful policy model is to think in four pillars. Together, they resemble an intelligence system. One layer gathers signals, another interprets them, a third connects decision-makers, and the last triggers action.
A policy taxonomy that decision-makers can use
Some remote diagnostics begin with a clinician. Others begin with a sensor, a kit, or software. What matters for governance is the function each performs.
| Technology Pillar | Primary Function | Example | Typical Use Case |
|---|---|---|---|
| Data Collection & Transmission | Capture patient information remotely and send it securely | Home monitoring device or wearable sensor | Ongoing observation outside hospital |
| Analysis & Interpretation | Turn raw data into clinically usable insight | AI-supported image or signal review | Triage, pattern recognition, risk flagging |
| Communication & Consultation | Connect patient and clinician for assessment | Video consultation platform | Remote review and decision-making |
| Intervention & Management | Enable treatment adjustment or care escalation | Virtual ward workflow or remote care plan delivery | Early response when deterioration is detected |
The first pillar is data collection and transmission. This includes home devices, wearables, self-testing kits, and pre-hospital monitoring systems. These tools don't diagnose by themselves in a policy sense. They generate the signal.
The second is analysis and interpretation. Software, clinical rules, and increasingly AI convert signal into meaning. An ECG trace, an image, or a symptom pattern only becomes useful when a clinician or validated system can interpret it reliably.
Why these pillars need common data architecture
The third pillar is communication and consultation. This pillar encompasses secure messaging, video review, and digital triage platforms. The diagnostic process often still depends on dialogue, judgement, and context.
The fourth pillar is intervention and management. This is the least discussed and the most important for ministers. A remote diagnostic pathway only creates value if it can trigger action, such as escalation to urgent care, medication review, virtual ward admission, or a change in management.
Practical rule: If a government procures only the first pillar, it buys data noise. If it procures all four, it buys a care pathway.
That's why data architecture matters so much. Many failures in remote diagnostics aren't failures of sensing or software. They are failures of integration. When policymakers need a practical primer on how data moves from fragmented clinical systems into common analytical environments, the OMOPHub guide to healthcare ETL offers a helpful technical overview of standardisation choices that sit beneath interoperability policy.
A mature national strategy doesn't ask, “Which app should we buy?” It asks, “How do these four pillars connect under a common governance model?”
Global Use Cases and Strategic Impact
Remote diagnostics are becoming part of national health infrastructure, not a niche digital add-on. For G7 and G20 governments, the strategic question is no longer whether these tools can work. It is where they create the highest public value, and which governance choices determine whether that value is captured domestically or ceded to external vendors and fragmented standards.

From outbreak control to routine care
The clearest lesson from recent adoption is that remote diagnostics perform best when governments treat them as part of a system-wide operating model. During outbreaks, they support case identification, triage, follow-up, and public health reporting without requiring every patient interaction to pass through a clinic or hospital. In routine care, the same architecture can support home monitoring for long-term conditions, pre-consultation assessment in primary care, and earlier escalation when risk begins to rise.
That shift matters for state capacity.
A remote diagnostic pathway can reduce pressure on physical sites, but its larger strategic effect is more selective use of scarce clinical labour. Systems that can review symptoms, images, or physiological signals before an in-person visit are better placed to reserve hospital attendance for high-acuity cases and procedural care. That is a service redesign question, not only a procurement question.
Emergency and pre-hospital care show the same pattern. If ambulance teams or urgent care services can transmit clinically usable data before arrival, hospital teams can prepare earlier and make faster decisions at handover. The gain is not speed alone. It is a more informed allocation of beds, specialists, and diagnostic resources across the pathway.
The policy implication is straightforward. Remote diagnostics create the greatest return when they are linked to decisions about triage, referral, and treatment, rather than funded as stand-alone devices or apps.
To see the broader clinical context in visual form, this short briefing captures how virtual consultation and digital pathways are increasingly tied to assessment, escalation, and continuity of care.
Why ministers should care about the operating model
Ministers should view these use cases through a strategic lens. The same core capabilities often underpin infectious disease surveillance, remote chronic disease management, virtual urgent care, and specialist review across distance. That common substrate includes trusted data exchange, clear clinical accountability, reimbursement rules that support remote activity, and workforce arrangements that allow expertise to move to the patient rather than the reverse.
This is also why data governance has become a strategic health policy issue rather than an IT concern. A useful primer on that wider shift is this analysis of why health data governance is everyone's business. Countries that organise diagnostic data as a national asset can improve service planning, quality assurance, and public health response. Countries that leave adoption to disconnected pilots usually get patchy coverage, inconsistent quality, and weak bargaining power with suppliers.
Three strategic impacts stand out:
- Stronger public health operations: Governments can identify, monitor, and route cases through digital pathways that complement laboratory and clinical infrastructure.
- Better continuity between encounters: Care teams can review change over time instead of relying on episodic in-person contact after deterioration is already visible.
- Tighter control of system capacity: Hospitals and specialist services can prioritise in-person slots for patients who need procedures, imaging, or high-touch assessment.
A second order effect deserves more attention in G7 and G20 discussions. Remote diagnostics can either reduce geographic inequality or harden it. If reimbursement, connectivity, and licensure rules are aligned, specialist interpretation can reach underserved regions. If those enablers are absent, wealthier urban providers adopt first and peripheral systems fall further behind. For policymakers examining how licensing architecture affects cross-jurisdiction care delivery, Understanding interstate licensure compact offers a practical reference point.
The strongest national strategies therefore judge remote diagnostics by institutional impact. They ask whether the technology improves surveillance, allocates workforce more intelligently, and protects equitable access across regions. That is the level on which multilateral coordination becomes relevant.
The Governance Challenge of Cross-Border Hurdles
The international challenge isn't invention. It is alignment. Remote diagnostic technologies increasingly move across jurisdictions through software, cloud infrastructure, specialist review, and multinational suppliers. Yet their governance remains nationally fragmented.

Regulatory fragmentation is now a growth constraint
A device, algorithm, or remote care workflow that is acceptable in one system may face a fresh approval, liability, or reimbursement hurdle in another. That slows diffusion and raises costs for both suppliers and public systems. It also creates a quiet strategic risk. Larger markets can shape de facto standards, while smaller systems become rule-takers.
This is not unique to diagnostics. Similar frictions appear in medical licensure and cross-jurisdiction practice. For policymakers looking at how subnational and interstate rules can either ease or complicate remote care, the WeekdayDoc explainer on the interstate licensure compact is a useful analogue for how governance architecture affects practical scaling.
A G7 or G20 dialogue should focus less on full legal uniformity and more on mutual recognisability. If countries can align baseline expectations for validation, auditability, and post-market oversight, they can lower the administrative burden without lowering standards.
Data sovereignty and trust are not secondary issues
Remote diagnostics often depend on patient data moving for specialist review, software support, or model improvement. Once that data crosses borders, three questions arise immediately. Who governs access? Which legal regime applies? Who is accountable if the data is misused or the model performs unevenly?
These aren't abstract concerns. They shape whether ministries, clinicians, and patients trust the system at all. The wider policy debate on health data governance already shows why this matters, as argued in health data is everyone's business.
Trust in remote diagnostics is built less by marketing claims than by visible rules on data use, review, and redress.
Countries also need to think carefully about representativeness. A tool trained or validated in one population may not translate cleanly to another care setting. Even where the technology is strong, the governance burden remains. Cross-border deployment should trigger stricter scrutiny of context, not weaker scrutiny because a product is already in use elsewhere.
Interoperability is a political choice
Many leaders still treat interoperability as a technical back-office matter. It isn't. It is a procurement decision, a standards decision, and often a sovereignty decision.
When remote diagnostic tools cannot exchange data cleanly with electronic records, ambulance systems, laboratory pathways, or public health reporting structures, value leaks out of the pathway. Clinicians duplicate work. Patients repeat information. Suppliers gain an advantage through lock-in. Ministries lose visibility over system performance.
The practical policy levers are well known, even if implementation remains difficult:
- Require open standards in procurement: Governments can make interoperability a condition of public purchase.
- Set portability rules for clinical data: Patients and providers should be able to move information without prohibitive friction.
- Create conformance testing regimes: Standards only matter if systems are tested against them.
The countries that lead here won't necessarily be those with the most apps. They'll be the ones that make cross-system coordination boring, dependable, and routine.
Bridging the Gaps in Equity Workforce and Finance
The public narrative around remote diagnostics often assumes that digital delivery is automatically more inclusive, more efficient, and easier to scale. In practice, each of those outcomes depends on policy design. Without that design, remote diagnostics can sharpen existing divides.
Equity fails first when access is assumed
A remote pathway is only accessible if the patient can use it, afford the connectivity around it, and trust that it will lead to care rather than delay. Older adults, rural populations, low-income households, and people with limited digital confidence often face the highest barriers.
That means equity policy cannot sit outside digital health policy. It has to be built into service specification from the start.
Key ministerial questions include:
- Access design: Can patients move easily between remote and in-person channels?
- Language and usability: Are instructions, interfaces, and escalation points understandable?
- Connectivity support: Are services being commissioned in areas with weak digital access?
A remote service is not equitable because it is available online. It is equitable when patients can enter and benefit from it on fair terms.
Clinical workforce models still lag behind the technology
Technology now captures more patient data outside clinical settings. Many workforce models still assume care happens mainly inside appointments. That mismatch creates operational strain.
Clinicians need time, workflow clarity, and accountability structures for reviewing incoming data. Managers need escalation rules that prevent alert overload. Professional education needs to prepare staff for care pathways built around continuous or near-real-time observation rather than episodic contact.
This challenge is governance-intensive, not just technical. It touches role design, indemnity, supervision, and service planning. A ministry can fund devices and still fail if frontline teams don't know who is supposed to act on the information they generate.
Finance determines whether pilots become public service
The financing problem is often the decisive one. Pilots attract innovation funding because they are visible and politically attractive. Long-term reimbursement is harder because it requires commissioners to pay for workflow redesign, staff capacity, digital support, and ongoing oversight.
The NHS England virtual wards programme shows the gap between ambition and operational scale. The programme reported over 10,000 beds in use in 2024, while the NHS Long Term Plan had committed to 40 to 50 virtual ward beds per 100,000 population by 2023/24, indicating a substantial implementation gap rather than a simple policy endorsement (BMJ Open analysis via PubMed Central).
This is the caution for G7 and G20 governments. Even where political support is strong, scaling remote diagnostics depends on mundane public finance questions:
- Who pays after the pilot ends
- Which provider is responsible for monitoring
- How outcomes are measured for reimbursement
- What support is available for digitally excluded patients
An integrated strategy doesn't separate these questions. Equity, workforce readiness, and financing rise or fall together.
Case Study The UKs Integrated Diagnostics Model
The UK case shows that remote diagnostics become strategically important only when government treats them as a system reform, not a device rollout. For G7 and G20 policymakers, the lesson is practical. Scale comes from aligning procurement, clinical pathways, data governance, and industrial policy inside one public architecture.
That is why the UK matters beyond its own health system. The NHS has pursued remote diagnostics as part of wider service redesign, linking them to urgent care, virtual wards, and digitally enabled chronic disease management rather than isolating them as a telehealth add-on.
What the NHS model gets right
A first strength is institutional integration. In the UK model, remote monitoring is tied to defined services, referral routes, and escalation protocols. Devices generate value only when clinicians receive interpretable data, know who is responsible for review, and can act within an agreed timeframe. This sounds administrative. It is, in fact, the difference between a pilot and a functioning national service.
A second strength is policy coherence. The NHS has combined demand-side purchasing power with standard-setting and pathway redesign. That gives suppliers clearer signals about what public systems will pay for: interoperability, clinical reliability, and compatibility with existing care delivery. Countries examining the wider remote diagnostic technologies policy debate should pay attention to that governance choice, because it shapes markets long before formal industrial strategy does.
The strategic implication is often missed. Public health systems do not just adopt remote diagnostics. They determine which types of innovation become commercially viable.
What other countries should copy carefully
The UK is also a useful case because it shows where higher-value capability sits. Philips' acquisition of the UK-based company Remote Diagnostic Technologies pointed to national strengths in pre-hospital monitoring, cardiac therapy, data management, and emergency workflow integration, all areas where interoperability and low-latency data transmission matter for clinical use (Philips announcement on acquiring Remote Diagnostic Technologies).
This matters for G7 and G20 strategy. Much of the public discussion still focuses on consumer-facing apps and basic virtual consultations. The UK experience suggests that the larger long-term opportunity lies in integrating diagnostics into ambulance services, hospital-at-home models, specialist monitoring, and emergency response systems. Those segments are harder to build, but they create stronger public value and greater resilience benefits.
Two policy lessons follow.
First, public procurement can shape innovation trajectories across borders. If governments specify open standards, device compatibility, and workflow integration in contracts, manufacturers have incentives to design for health system use rather than short-term consumer uptake.
Second, integration is slower than acquisition. Governments can buy hardware quickly. Building trusted pathways for triage, escalation, liability, and cross-provider coordination takes sustained institutional work. The UK model is instructive because it demonstrates both progress and constraint, which makes it more useful for ministers than a simple success narrative.
A G7/G20 Roadmap for Secure and Equitable Adoption
The next phase requires political coordination. Remote diagnostics have reached the point where isolated national experimentation is no longer enough. G7 and G20 leaders should treat them as a shared governance agenda tied to resilience, preparedness, and inclusive access.
Four actions for leaders
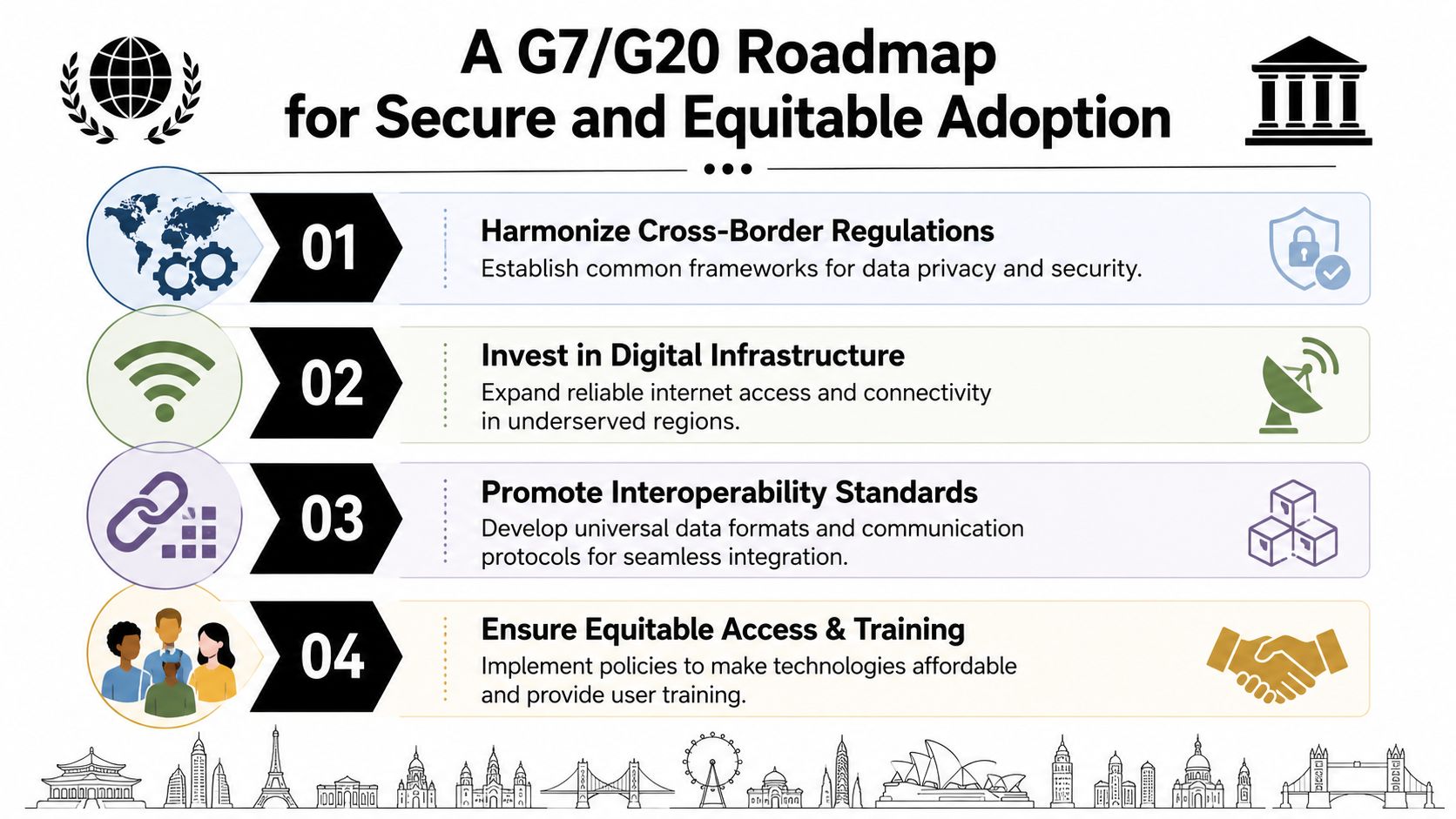
A workable roadmap should prioritise four actions.
Create a standing G20 coordination mechanism on remote diagnostics. Its purpose should be practical. Align evidence expectations, post-market monitoring principles, and baseline rules for cross-border deployment.
Use procurement to force interoperability. Governments are major buyers. They can require open standards, portability, and conformance testing instead of rewarding proprietary lock-in.
Tie digital expansion to equity obligations. Any national strategy should include support for connectivity, non-digital alternatives, and patient enablement. Otherwise, the benefits will concentrate where infrastructure is already strongest.
Shift from pilot logic to pathway finance. Reimbursement should cover the full operating model, including monitoring, review, escalation, and technical support.
What success looks like in practice
The UK experience with remote patient monitoring points to the practical model ministers should back. Wearable and home devices can stream physiological data to clinicians, enabling earlier intervention and helping prevent avoidable hospitalisations, but success depends on reliable data infrastructure and workflow integration rather than devices alone (remote patient monitoring and data flow in practice).
That is the central policy lesson. Remote diagnostics work when governments govern the pathway, not just the product.
For G7 leaders in particular, the strategic case is broader than national efficiency. Shared action on standards, safety, and inclusive implementation would reduce duplication, accelerate trusted adoption, and strengthen multilateral cooperation around digital health. This argument sits squarely within the wider case for why the G7 must act now to address the digital health transformation.
The winning countries won't be those with the most remote diagnostic tools. They'll be those that make those tools accountable, interoperable, and usable at population scale.
The window for shaping the rules is open now. If G7 and G20 governments act together, remote diagnostic technologies can help build a health system that is more distributed, more resilient, and more equitable than the one the pandemic exposed as too brittle.
Global Governance Media convenes leaders and policy communities around the choices that will shape global health, digital governance, and multilateral cooperation. If you want sharper analysis on the G7 and G20 agenda, follow Global Governance Media for evidence-based briefings, expert commentary, and practical policy roadmaps.